
This article was last updated on February 10, 2025.
What is UDI?
UDI systems are intended to benefit healthcare providers, manufacturers, authorized health authorities, hospitals and institutions, and individual consumers by providing:
- Faster discovery of possible flawed medical device information by health authorities.
- Quicker access to recall information, and visibility into current inventory.
- A reduction in medical errors through consistently documented product expiration dates.
- Identification of any counterfeit products being used in healthcare facilities.
- Assurances that information regarding an implanted device is safely retained and traceable.
UDI timelines and deadlines vary by market, classification risk, and product and have been revised multiple times in some countries*. This article details the UDI deadlines for the countries which have announced specific programs (draft or implemented) and is current as of the date of this article.
*Note: these dates can change as participating countries adjust their plans. We do our best to update this as more information becomes available.
Quick Links to country-specific sections:
- Australia UDI
- Brazil UDI
- Canada UDI
- China UDI
- European Union UDI
- India UDI
- Japan UDI
- Saudi Arabia UDI
- Singapore UDI
- South Korea UDI
- Taiwan UDI
- United States UDI
- UDI databases by country
General UDI labeling requirements
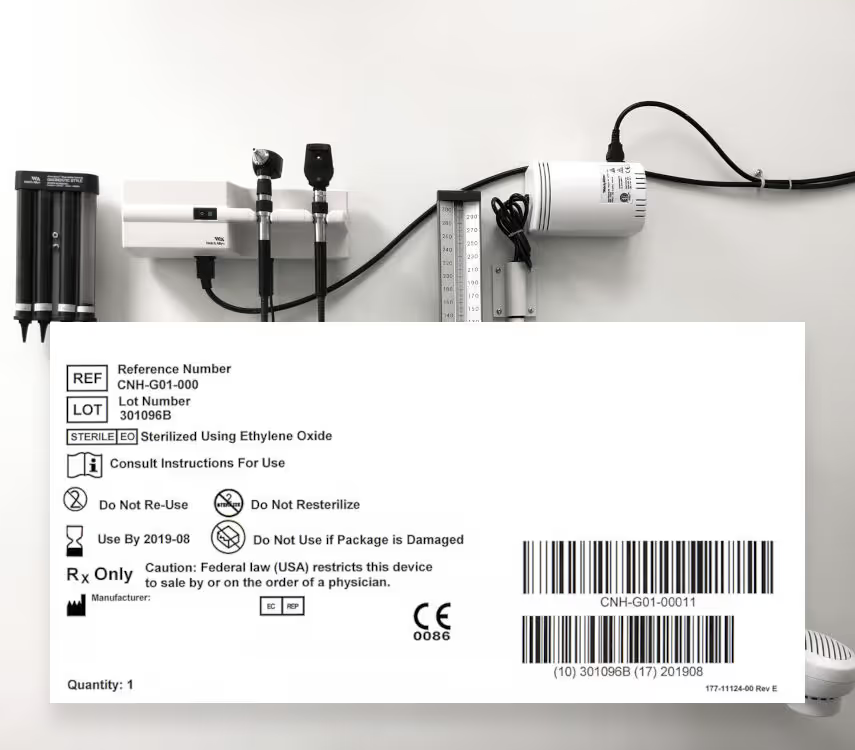
There are two components to a medical device UDI: the UDI device identifier (UDI-DI) and the UDI production identifier (UDI-PI). The UDI is presented as a barcode label (human and machine readable) on device packaging or on the device itself and acts as the access key to all device UDI attributes.
UDI-DI: This is the static portion of the UDI which identifies the manufacturer along with the specific device version. The UDI-DI (device identifier), also known as the Global Trade Item Number (GTIN) is assigned by an approved organization, such as GS1, and contains:
- Company prefix
- Manufacturers internal product code
- Check character
The UDI-DI is the primary identifier to be used in looking up device attributes in country-specific databases and is assigned prior to placing a product on the market. Note that the device identifier is different for different packaging levels of the same device.
UDI-PI: This is the dynamic portion of the UDI which is assigned by the manufacturer and identifies one or more of the following:
- Manufacturer’s lot or batch number
- Serial number
- Manufacturing date
- Expiration date
- Other attributes as defined by country-specific regulations
The UDI-PI actual values do not appear in country-specific databases (with the exception of the EU vigilance database).
Australian UDIGuidelines
Reporting Database: AusUDID (pre-production)
The Australian government for medical devices, the TGA, has not launched any official regulations or timeline for mandatory UDI labeling. They do provide a wealth of information on their website that is worth reviewing. In the meantime, however, they are hoping for a Q1 2025 implementation. The AusUDID Pre-Production environment is available for sponsors and manufacturers of medical devices supplied in Australia. It is a test environment that allows testing of data submission, prior to submission to the AusUDID Production environment. Any sponsor or manufacturer with an active TBS account can access the database.
ANVISA UDI guidelines
Reporting database:TBD
RDC No. 591/2021 is the regulations guideline for the identification of medical devices regulated by ANVISA, implementing the Unique Identification of Medical Devices (UDI) system. In July 2024, ANVISA finalized amendment RDC No. 884/2024 which implemented various adjustments to RDC 591/2021. The biggest take-away regarding UDI is the extension of one year on the implementation deadlines.
Health Canada website
Reporting Database: N/A
Position paper on the current state of UDI implementation
Medtech Canada strongly supports the global initiative led by regulators under the guidance of the International Medical Devices Regulators Forum (IMDRF), which aims to standardize the identification of medical devices by requiring that certain medical devices carry an internationally recognized UDI. Currently, there is no process in place for UDI in Canada.
China (NMPA) website
Reporting Database: China National UDI Database
Announcement No 22 of 2023
On January 1, 2021, the NMPA implemented the UDI system for its first batch of medical devices, including 69 Class III devices. The following year, June 1, 2022, followed the implementation for the second batch of other Class III medical devices (including IVD reagents). Then in 2023, Order No. 22 announced the third batch of products to adopt the UDI system.
As of June 1, 2024, medical devices listed in the third batch implementation product catalog must have already had UDI implemented. According to the degree of risk and regulatory needs, some Class II medical devices in the third batch included high-demand single-use products, items selected for centralized procurement, and medical aesthetic products, totaling 103 types in 15 categories.
European Union UDI Information
Reporting Database: EUDAMED
Rimsys Updated EUDAMED Timeline Blog Post
The UDI & Devices module is expected to be declared fully functional by the end of Q2 2025 and mandatory for industry use on January 1, 2026. The EU continues to strongly recommend to the industry to establish its solution and to submit data on a voluntary basis.
Medical Devices Rules, 2017
Legal Metrology Act, 2009
Reporting Database: N/A
Rule 46 of Medical Device Rule 2017 was set to require UDI labeling by January 1, 2022. However, details on how the UDI needs to be implemented have not yet been released but India's labeling and traceability requirements must be met as per CDSCO regulations.
In addition to the Medical Device Rule 2017, the Legal Metrology Act, 2009 focuses on standardizing weights and measures and ensures that packaged commodities, including medical devices, are labeled with accurate and clear information.
Law to Ensure Quality, Efficacy and Safety of Pharmaceuticals, Medical Device, and Similar Products
Reporting Database: N/A
There are two regulatory authorities responsible for regulation of medical devices in Japan: The Ministry of Health, Labour and Welfare (MHLW) and the Pharmaceuticals and Medical Devices Agency (PMDA). The MHLW is responsible for the administrative actions such as guidance and approval, and judgment on whether or not a product is considered a medical device. The PMDA undertakes product review and post-market safety measures.
As of Dec 2022, bar code labeling based on international standards is required for immediate containers/wrappings/retail packages of medical devices. It is expected for barcodes to be displayed on every medical device in unit of use for patients. Japan was an early promoter of standardized barcodes and is still working towards harmonizing the requirements with global UDI expectations.
The Pharmaceuticals and Medical Devices Act (PMD Act) translates in Japanese meaning "Law to Ensure Quality, Efficacy and Safety of Pharmaceuticals, Medical Devices, and Similar Products," but is often shortened to Act on Pharmaceuticals and Medical Devices or just PMD Act.
Requirements for Unique Device Identification (UDI for Medical Devices)
Reporting Database: Saudi-DI
The SFDA requires compliance with the Unique Device Identification (UDI) regulations on all medical device companies in Saudi Arabia for all classifications. Medical device classifications include: devices, IVD, non-medical IVD, chemical for medical use, distillation device, general lab use, HCT/Ps product and radiation devices.
Guidance for UDI Implementation
Reporting Databases: Singapore Medical Device Register (SMDR) - For risk class B or higher, Class A Medical Device Database - Risk class A only
Singapore is now requiring compliance with UDI labeling and database registration. They will accept UDI labels for devices already marketed in the U.S. and the EU without any need for modification. However, if they are not marketed in either country, then they are required to implement via Singapore UDI regulations.
Companies are given an additional 6 months from the compliance date to deplete the respective medical devices that have been imported prior to the compliance date and exist in their current supply chain.
Note:
• UDIs will not be required for medical devices for clinical research, investigational testing or clinical trial and custom-made medical devices
• Medical devices authorized for supply via Special Access Routes (GN26, GN27, GN29) are required to comply with UDI requirement on a risk-calibrated approach
Act on In Vitro Diagnostic Medical Devices
Act on Medical Devices
Reporting Database: South Korean Integrated Medical Device Information System (IMDIS)
South Korea has already implemented UDI regulations by Article 20-23 of the Medical Device Act (No. 14330) and Article 54-2 of Enforcement Regulations of Medical Device Act (No. 1512).
Guidance document from Taiwan FDA
Reporting Database: TUDID
Taiwan has previously implemented UDI regulations, which include labeling and database reporting requirements.
FDA website for UDI
Reporting database: GUDID database
The United States has previously implemented UDI regulations, which includes labeling and database reporting requirements.
Each country has their own UDI database and varying requirements for the data stored in those databases. There is overlap in the data required among the various UDI databases, but each country also has unique data they require.
In addition, countries require that UDI-DI information be provided by “issuing entities.” Note that with the exception of China, all countries accept GS1, HIBCC, and ICCBA as issuing entities.
* Data attributes are approximations based on country UDI requirements and include mandatory, optional, mandatory if applicable, and country database auto generated elements.
** Expected to be similar to US GUDID requirements.
Keeping pace with UDI regulations
Keeping track of country-specific UDI requirements, implementation timelines, and affected devices can be a big challenge to RA teams—especially because the information is scattered across many sources and simply hard to find. In this guide, we have consolidated timeline information and device class requirements across multiple countries. While we make every effort to provide accurate and up to date information, it's always advised to check the government website for the country in question.
Additional UDI resources
Looking for more information? You can visit our EUDAMED resource center, where you will find videos and resources to help you plan for UDI requirements in Europe. In addition, you may enjoy our blog post that outlines our views on the recent EUDAMED timeline updates.
For a broader introduction to UDI, see our Rimsys UDI Overview blog post.
If you're looking for an automated, integrated solution to help you meet changing regulations and manage your global UDI program, request a custom Rimsys demo!

GET IN TOUCH



.avif)
