


Featured
Rimsys Announces Rimsys AI to Eliminate Repetitive Tasks and Enhance Decision-Making for MedTech Regulatory Teams
Rimsys, the leading Regulatory Information Management (RIM) platform for the MedTech industry, today announced the launch of Rimsys AI, a suite of embedded artificial intelligence (AI) agents.

The beginner's guide to the FDA De Novo classification process
This article is an excerpt from The beginner's guide to the FDA De Novo classification process ebook.
Contents
- Introduction
- Chapter 1: What is an FDA De Novo request?
- Chapter 2: Contents of a De Novo request
- Chapter 3: Submitting a De Novo request
- Appendix A: Acceptance review checklist
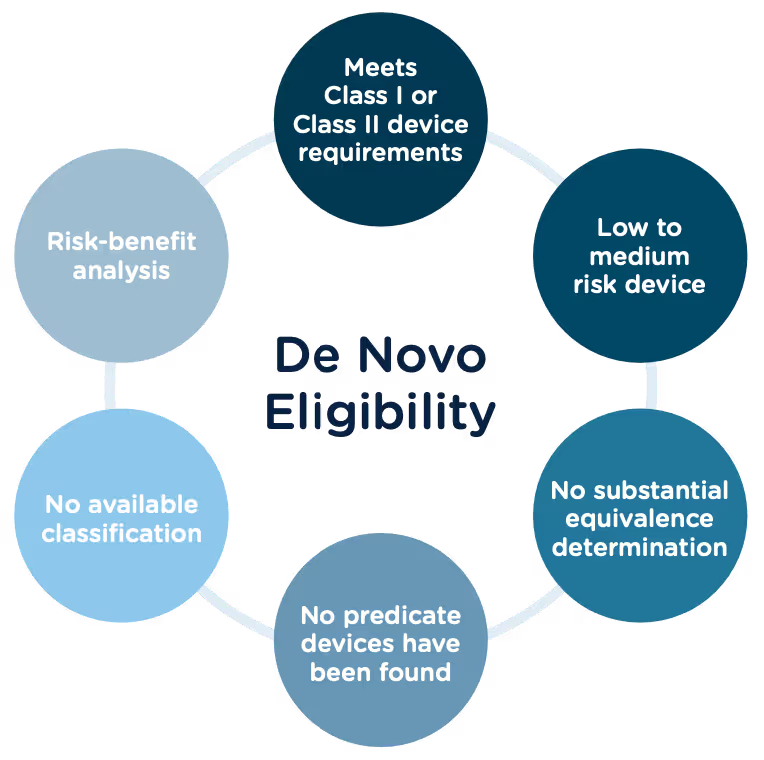
Congratulations, you have successfully developed a new medical device! Now you need to take it to market. Normally in the United States this would mean completing a 510(k) submission. However, the 510(k) relies on “substantial equivalence”—a comparison to a similar device already on the market (also called a predicate device) to assess the risk profile of the new device. What if your device is totally new, and there isn’t a similar device to compare it to? Enter the FDA De Novo process. The De Novo process provides a pathway to market for novel devices with a low to medium risk profile.
What does De Novo mean?
According to the Merriman-Webster dictionary, de novo is a Latin word meaning “as if for the first time; or anew.” Perfectly fitting that the FDA uses this term “De Novo” to describe market approval requests for new medical devices or technology where there is no comparable predicate device on the market.
The Food and Drug Administration Modernization Act of 1996 provided the FDA with the authority to create the De Novo Classification Process. It's a process that uses a risk-based strategy for a new, novel kind of medical device, in vitro diagnostic, or medical software solution whose type has previously not been identified and/or classified. It’s a process by which a novel medical device can be classified as a Class I or Class II device, instead of being automatically classified as Class III, which may not be appropriate. Before the implementation of the De Novo process in 1997, all the “not substantially equivalent” (NSE) products were required to be initially classified as a Class III device. But for a lot of devices, this risk class didn’t really make sense. The De Novo process provides a pathway for more accurate classifications of novel, lower-risk devices.
October, 2021, the FDA released a final guidance document "De Novo Classification Process (Evaluation of Automatic Class III Designation)" to provide guidance to the requester (also known as the manufacturer) and the FDA on the process for the submission and review of a De Novo Classification Request under section 513(f)(2) of the Federal Food, Drug, and Cosmetic Act (the FD&C Act). This process provides a pathway to an initial Class I or Class II risk classification for medical devices for which general controls or general and special controls, provide a reasonable assurance of safety and effectiveness, but for which there is no legally marketed predicate device. This guidance document replaced the "New Section 513(f)(2) – Evaluation of Automatic Class III Designation, Guidance for Industry and CDRH Staff" document, dated February 19, 1998.
Consistent with the final rule, the FDA updated the guidance documents below to provide recommendations for submitting De Novo requests, as well as criteria and procedures for accepting, withdrawing, reviewing, and making decisions on De Novo requests, effective January 3, 2022.
- User Fees and Refunds for De Novo Classification Requests
- FDA and Industry Actions on De Novo Classification Requests: Effect on FDA Review clock and Goals
- Acceptance Review for De Novo Classification Requests
The 510(k) and the De Novo processes are similar in that they are both pathways to market for medical devices with low to moderate risk, which is Class I and Class II. The biggest difference between the two is that the 510(k) heavily relies on the concept of "substantial equivalence" to an existing medical device. You must prove this to get the clearance of your 510(k) submission. In the De Novo process, there isn’t a product currently on the market that is “substantially equivalent” to yours, so it’s like starting with a clean slate. For more on the 510(k) process, see our Beginner’s Guide to the 510(k) ebook.
A result of the De Novo process to be aware of is that a successful submission will lead to a new predicate device type that someone else can reference to bring their product to market through the 510(k) process. You’ve done all the work, so now it’s available for anyone to use to provide "substantial equivalence".
De Novo history/timeline
Preparing a De Novo request
1. Do your research! Be sure to complete all the necessary research prior to your submission. You want to be sure that your device is not substantially equivalent to an existing device. Resources to review include:
- The Center for Devices and Radiological Health (CDRH)
- U.S. FDA Device Classification Database
- Device Classification Under Section 513(f)(2)(De Novo)
2. A De Novo request can be submitted with or without a preceding 510(k). There are two options for when you can submit a De Novo request:
Option A: After receiving a not substantially equivalent (NSE) determination (that is, no predicate, new intended use, or different technological characteristics that raise different questions of safety and effectiveness) in response to a 510(k) submission.
Option B: If you’ve determined, after extensive research, that there is no legally marketed device on which to base a determination of substantial equivalence.
3. Be sure all fees are paid to the FDA in advance of submitting a De Novo request. The FDA’s fiscal year begins in October and runs through the following September. Fees have increased each year since they were introduced, but the FDA’s percentage of reviews completed within the 150-day window has increased as well.
A business that is qualified and certified as a “small business” is eligible for a substantial reduction in most of the FDA user fees, including De Novo. The CDRH is responsible for the Small Business Program that determines whether a business is qualified.
Medical Device User Fee Amendments (MDUFA) guidance documents can provide more detailed information about all FDA user fees.
4. The initial request process serves only to determine if the De Novo request is administratively acceptable based upon the Acceptance Checklist. The initial acceptance is followed by substantive review which will determine the final risk classification of your device.
5. A Pre-Submission (Pre-Sub) is a formal written request for feedback from the FDA that is provided in formal written form, and then followed by a meeting. Although a Pre-Sub is not required prior to a De Novo request, it can be extremely helpful to receive early feedback, especially for devices that have not previously been reviewed under a 510(k). If you think you would like to submit a pre-sub first, there are suggested guidelines for submission you should consider:
- Describe your rationale for a Class I or Class II classification for your device.
- Provide the search results of FDA public databases and other resources used to determine that no legally marketed device and no classification for the same device type exists.
- Provide a list of regulations and/or product codes that may be relevant.
- Provide a rationale for why the subject device does not fit within and/or is different from any identified classification regulations, based on available information.
- Identify each health risk associated with the device and the reason for each risk.
- Briefly describe any ongoing and/or planned protocols/studies that need to be completed in order to collect the necessary data to establish the device’s risk profile.
- Provide information regarding the safety and effectiveness of the device. Cite the types of valid scientific evidence you anticipate providing in your De Novo request, including types of data/studies relating to the device’s safety and effectiveness.
- Briefly describe any ongoing and/or planned protocols/studies that need to be completed to collect the necessary safety and effectiveness data.
- Provide protocols for non-clinical and clinical studies (if applicable), including how they will address the risks you anticipate and targeted performance levels that will demonstrate that general controls or general and special controls are sufficient to provide reasonable assurance of safety and effectiveness.
- Share any proposed mitigation measure(s)/control(s) for each risk, based on the best available information at the time of the submission. Highlight which mitigations are general controls and which are special controls and provide details on each.
- Include any other risks that may be applicable, in addition to those identified in the Pre-Sub, given the indications for use for the device.
- If applicable, provide any controls that should be considered to provide a reasonable assurance of safety and effectiveness for the device.
- Provide any non-clinical study protocols that are sufficient to allow the collection of data from which conclusions about device safety and/or effectiveness can be drawn. These protocols should address whether the identified level of concern is the appropriate level of concern for the device software, and if any additional biocompatibility and/or sterility testing is required.
- If clinical data is needed, provide information to show that the proposed study design and selected control groups are appropriate?
6. The FDA will attempt to review the De Novo request submission within 15 calendar days of receipt of the request to make a determination that the submission is declined or accepted for review. If they are unable to complete the review within the 15 days, your submission will automatically move to “accepted for review” status. https://www.fda.gov/regulatory-information/search-fda-guidance-documents/de-novo-classification-process-evaluation-automatic-class-iii-designation
7. There are times when the FDA will refund your application fee. They have created a guidance document “User Fees and Refunds for De Novo Classification Requests” for the purpose of identifying:
- the types of De Novo requests subject to user fees
- exceptions to user fees
- the actions that may result in refunds of user fees that have been paid
When is a De Novo request subject to a user fee?
When will the FDA refund a De Novo user fee?
What fee must be paid for a new device submission following a De Novo “decline” determination?
To continue reading this eBook including a detailed walk-through of all the Traditional 510(k) components, submission requirements and timelines, and an overview of the other 510(k) forms including the Abbreviated 510(k) and the Special 510(k), please register to download the full version.




MedWatch: The FDA safety information and adverse event reporting program
What is MedWatch?
What should you do if you encounter a serious side effect from a prescription drug you've taken? Or what if you were using a medical device and it malfunctioned and caused you serious harm? Do you contact the manufacturer, your doctor, or your local government? The quick answer is to contact the FDA, and it’s not as complex as you may think.
In the early 1990s, the FDA knew it needed a reliable way to help physicians, health care workers, and all those who work in the medical field to report adverse events related to pharmaceuticals and medical devices. An adverse event is any undesirable experience associated with the use of a medical product or pharmaceutical drug. They wanted a system that could be used to track these events and give them the insight they needed to review and track the reported issues.
In 1993 the FDA introduced the MedWatch program designed to collect voluntary reports of adverse reactions and quality problems of drugs and medical devices, along with all other FDA-regulated products such as dietary supplements, cosmetics, pet food, toys, tobacco, infant formulas, etc. The Stakeholder Engagement Staff within the office of the FDA commissioner is ultimately responsible for this program. They work closely with all FDA centers and offices across the entire agency and serve as a liaison between stakeholder organizations and the general public. In addition, it is their responsibility to report on medical product safety alerts, recalls, statements, and periodic safety labeling change summaries.
MedWatch is not only for medical professionals to report adverse events, but the public is also encouraged to report adverse events as well. And reporting an event to the FDA may be easier than you may think.
MedWatch Reporting
When the FDA approves a medical drug or product, the agency has determined that the benefits of the product outweigh the risks. But, sometimes there are unforeseen risks that are discovered once a product or drug gets to market and people start using it. For example, a product may be used by a larger and more diverse group of people than was represented in the clinical testing. They may differ in the complexity of their health problems or other medications that they use. Because of these unanticipated events, the FDA encourages people to report problems they feel that they’ve experienced.
To report a voluntary event online, you can use the MedWatch Online Voluntary Reporting Form 3500B, which is located on the FDA’s website. Form 3500B is a consumer-friendly reporting form that contains less technical language than the online FDA Form 3500, which is to be used by healthcare professionals. The form will step you through the process and should take about 15-20 minutes to complete. You can submit your contact information (in case they have questions or need clarification) or you can request that your information be kept confidential.
What happens after a report is made to MedWatch?
- FDA staff enter the report into a database so that it is available for review and comparison to other reports.
- An FDA safety evaluator, often a pharmacist, doctor, or nurse, reviews the report and examines the database for similar reports.
- The FDA monitors the data for trends and investigates, if appropriate.
- The FDA takes necessary action to protect public health.
Examples of FDA actions that could result from a report include:
- issuing safety alerts with recommendations to monitor a product's use, adjust the way it is used, or stop using it
- updating the product labeling to reflect new warnings
- inspecting the manufacturer
- requesting a change in the product’s design, manufacturing process, packaging, or distribution
- requesting that a company recall a product
MedWatch is a safety tool for everyone to use. Every MedWatch report is important and is recorded in an FDA database for review and comparison to similar previous reports. Taken together, these reports can identify trends and signal safety problems, leading to an FDA action to protect the public. Remember, reporting can help you, a family member, or someone else avoid harm, serious illness, or even death.
For more information, refer to the FAQ’s on the FDA website.
Join the MedWatch e-mail list here
An overview of 21 CFR Part 820
What is 21 CFR Part 820?
21 CFR 820 is the FDA federal regulation that pertains to quality systems for medical device manufacturers, and it is part of the agency’s set of Current Good Manufacturing Practices (CGMP) for industry. Also referred to as the FDA’s quality system regulation (QSR), the regulation defines design controls and quality processes at all stages of device development in order to ensure that all medical devices marketed in the United States are safe and effective.
21 CFR 820 consists of 15 subparts, which define quality system requirements for each stage and function within the medical device manufacturing process. We define each subpart below.
Federal regulations are organized as Title → Chapter → Subchapter → Part, which means that 21 CFR 820 is short-hand for:

21 CFR 820 vs ISO 13485
ISO 13485 is the de facto international quality system standard for medical device manufacturers, but this is not currently the standard in the United States. While Part 820 and ISO 13485 are structured differently, they have no conflicting requirements. Therefore, companies that are marketing medical devices in the U.S. and in other markets will need to comply with both ISO 13485 and the FDA’s QSR, as defined in 21 CFR 820.
However, the FDA is moving towards harmonizing these standards, and on February 23, 2022 issued a proposed rule to amend the QSR to align more closely with the international consensus standard for Quality Management Systems, primarily by incorporating reference to the ISO 13485 standard. The FDA has published FAQ’s about the proposed rule.
21 CFR Part 820 Requirements
Part 820: General Controls (subpart A)
The General Controls subpart contains three sections providing general information about the regulation, including the scope and applicability along with key definitions.
Scope
The regulation defines current good manufacturing practice (CGMP) requirements governing the methods, facilities, and controls used for the “design, manufacture, packaging, labeling, storage, installation, and servicing of all finished devices intended for human use." Specifically, this subpart defines:
- Applicability:
The requirements of this regulation are intended to ensure the safety and efficacy of all finished medical devices intended for human use that are manufactured in or imported into the United States. Manufacturers that are involved in some, but not all, manufacturing operations should comply with those requirements that are applicable to the functions they are performing.
Exceptions:
- This regulation does not apply to manufacturers of medical device components, but such manufacturers are encouraged to use this regulation as guidance.
- Class I medical devices are exempt from the Design Controls defined in this regulation, except for those listed in § 820.30(a)(2).
- Manufacturers of blood and blood components are not subject to this regulation but are subject to Biologics good manufacturing practices as defined in Subchapter F, Part 606 of the regulation.
Definitions
This section of the regulation contains definitions for a number of terms used throughout the document. The following are the major definitions related to quality records:
- Design history file (DHF): A compilation of records that describes the design history of a finished device.
- Design input: The physical and performance requirements of a device that are used as a basis for device design.
- Design output: The results of a design effort at each design phase and at the end of the total design effort. The finished design output is the basis for the device master record. The total finished design output consists of the device, its packaging and labeling, and the device master record.
- Device history record (DHR): A compilation of records containing the production history of a finished device.
- Device master record (DMR): A compilation of records containing the procedures and specifications for a finished device.
Quality System
The section of the regulation sets the basic requirement for a quality system by stating that “Each manufacturer shall establish and maintain a quality system that is appropriate for the specific medical device(s) designed or manufactured, and that meets the requirements of this part.”
The term “appropriate” is used throughout this regulation and can be open to interpretation. A manufacturer, however, should assume that all requirements are appropriate and applicable except in cases where non-implementation of the requirement can be shown to have no effect on the product's specified requirements or ability to carry out necessary corrective actions.
Quality system requirements (subpart B)
This section of the regulation defines the overall responsibilities and the resources required for the management of the quality system.
Management responsibilities
Executive management is responsible for establishing a quality policy and ensuring adequate resources to effectively maintain and manage the quality system. In addition, management is responsible for establishing a specific quality plan, consisting of relevant practices, resources, activities, and procedures.
Quality audit
Periodic audits of the quality system are required to be conducted by personnel not directly responsible for the activities being audited. The dates and results of each audit need to be documented, along with the results of the audit. It is expected that corrective actions and, when necessary, reaudits, be performed for any identified noncompliances.
Personnel
Manufacturers are responsible for assigning sufficient personnel with appropriate experience and training to perform all tasks required by the quality system plan.
Design controls (subpart C)
Manufacturers of all class II and class III medical devices, along with the specific class I devices listed in paragraph (a)(2) of this regulation, are required to establish design control procedures that ensure design requirements are met as specified.
Design controls shall define:
- Design and development planning - Plans that describe the design and development activities, and responsibilities for these activities and their implementation.
- Design input - Procedures that ensure design requirements are appropriate and address the intended use of the device.
- Design output - Procedures that document design output, including acceptance criteria, so that conformance to design input requirements can be adequately evaluated.
- Design review - Formal and documented reviews of the ensign results that include participation from representatives of all.
- Design verification - Procedures for verifying the device design that confirm that the design output meets the design input requirements.
- Design validation - Procedures for validating the device design, ensuring that devices conform to defined user needs and intended uses, and including testing of production units under actual or simulated conditions.
- Design transfer - Procedures to ensure that the device design is correctly translated into production specification.
- Design changes - Procedures for identifying, documenting, validating, and managing the verification and approval process of all design changes before they are implemented.
- Design history file - A design history file (DHF) is required for each type of device and should include or reference the records necessary to demonstrate that the design was developed in accordance with the approved design plan and device requirements.
Document controls (subpart D)
Medical device manufacturers are required to put in place document controls for all documents required in this regulation.
Document approval and distribution
One or more people must be assigned to review and approve documents prior to issuance. The approval must be documented, include a date and the signature of the approver, and be made available at all locations where applicable. Procedures must also be in place to ensure that obsolete documents are removed and/or prevented from being used.
Document changes
Similar to document approval procedures, changes to documents must be approved, reviewed, and documented. Records of all changes must be maintained.
Purchasing controls (subpart E)
To continue reading this Regulatory Brief, including a definition of the remaining subparts and a comparison of 21 CFR 820 to ISO 13485, please download the full brief.

What is the FDA eSTAR program?
History
In September of 2018, the FDA took their first step in their commitment to improve the process of a 510(k) electronic submission. This commitment was established as part of the Food and Drug Administration Safety and Innovation Act (FDASIA) that was enacted on July 9, 2012, amending the FD&C Act by adding section 745A.
Based on the FDA’s experience with the original eSubmitter process, the Center for Biologics Evaluation and Research (CBER) group piloted a slightly different program and called it the Electronic Submission Template and Resource Pilot Program, thus creating eSTAR. This second attempt at electronic submissions consists of a collection of questions, text, and prompts within a PDF template that guides a user to a ‘complete’ 510(k) electronic submission.
The FDA’s goal of this process is to enhance the quality of submissions by helping to ensure consistent, quality, comprehensive data for the Center for Disease and Radiological Health (CDRH) premarket review. With a standardized format in place, submitters of a 510(k) or De Novo can ensure that their submissions are complete and premarket reviews will be more efficient.
eSTAR timeline
.jpeg)
eSTAR Requirements
Currently, eSTAR is a voluntary process that will become mandatory starting October 1, 2023. It is free to use by medical device applicants wishing to submit a 510(k) or a De Novo to the CDRH, but is not to be used for combination products. Although it’s currently free to use, the standard submission fees for 510(k) and De Novo still apply.
A Refuse to Accept (RTA) review (a preliminary review used to ensure the submission is complete) will not be conducted on submitted eSTAR templates as the eSTAR template replaces this checklist and will state if the template is complete or incomplete on the first page. If the eSTAR does not have a completed status, it will not be reviewed by the FDA.
Guidance Information
The FDA has provided final guidance documentation in “Providing Regulatory Submissions for Medical Devices in Electronic Format — Submissions Under Section 745A(b) of the Federal Food, Drug, and Cosmetic Act” (referred to as the “745A(b) device parent guidance”). This guidance document provides a process for the development of templates to facilitate the preparation, submission, and review of regulatory submissions for medical devices solely in electronic format.
The FDA then provided final guidance in “Electronic Submission Template for Medical Device 510(k) Submissions.” There are exemptions listed in the guidance document that may allow users in certain situations to be exempted from eSTAR.
eSTAR Templates
The two templates provided by the FDA are PDF forms that can be filled out and saved, with attachments. The image below shows the device description page of the non-IVDR form. When using the form, red bars will appear in front of any required questions that have not yet been answered. Bars will turn green when all associated questions in a section have been completed. Gray bars indicate an optional question.
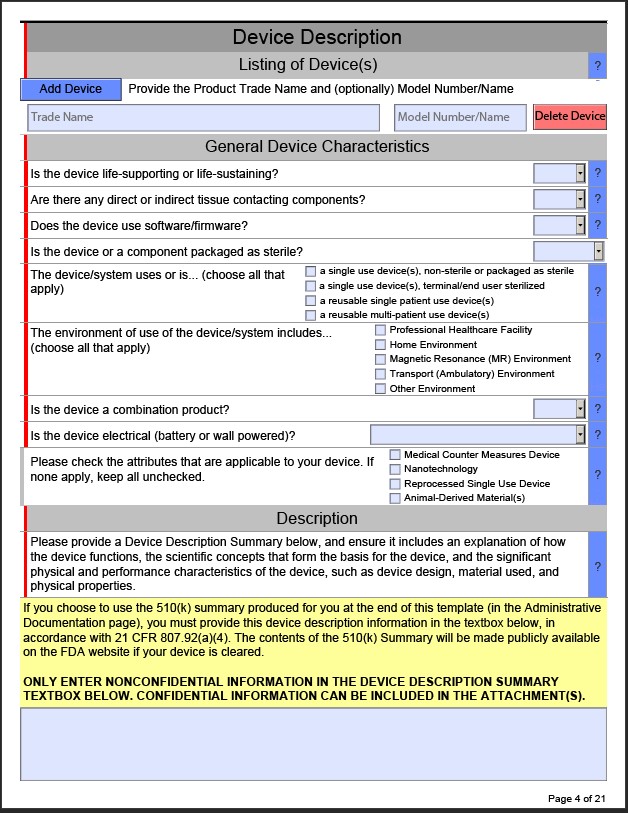
As questions are answered, additional dropdowns may appear that can require users to add additional information. For example, in the Pre-Submission Correspondence and Previous Regulatory Interaction Section within the non-IVD template, if you Select “Yes” the PDF will then add a section where you will need to add the Submission, Submission Number, and copies of the correspondence.
Pop-ups with useful information may also appear. For example, within the non-IVD template, in the General Device Characteristics Section, if a user selects that a device is a single use device, non-sterile or packaged as sterile, a Java Script window will appear with FDA guidance.

A note on embedded attachments: Any embedded attachments may only be used once per eSTAR PDF. You may need to “break up” documentation to fit the eSTAR template requirements if your testing reports cover multiple tests in one document.
What’s involved in a submission?
There are currently two processes for submission:
- The Customer Collaboration Portal
- Mailing the eCopy (CD, DVD or USB drive) containing the eSTAR PDF
First, effective July, 2022, The Customer Collaboration Portal was made available to existing users of the portal if they are the official correspondent of an organization and have also received the FDA email letting them know that they’re eligible.
The second method consists of a printed cover letter with an accompanying eCopy (CD, DVD or USB drive) containing the eSTAR PDF. Note that if the PDF submission exceeds 1 GB in size, it could delay the process, so high-resolution videos and images should only be included when necessary.
- Download the specific eSTAR PDF template for an In Vitro or Non-In Vitro device (see "Current eSTAR versions" section on this linked page).
- Fill out the template accordingly but note that it is only used for constructing - not submitting - your submission.
- The eSTAR does not need to comply with the FDA’s eCopy Guidance document, however, any additional files that are provided with the eSTAR PDF submission will need to comply with it. The FDA strongly recommends not providing additional files with the eSTAR PDF, though, as you already will be embedding your documents within the eSTAR template itself.
- You do not need to provide an Indications for Use page, the Premarket Review Submission Cover Sheet, or a Declaration of Conformity (if applicable) with your submission since they are already built into the eSTAR PDF. An additional option is to also build the 510(k) summary within the template itself instead of writing one.
An eSTAR submission will contain a larger number of files (as they will be embedded in the PDF eSTAR template) than traditional submissions, which are usually combined into one PDF file. We recommend preparing your entire submission before filling out the eSTAR template to minimize the need for reworking the submission.
A note on 510(k) product change submissions: The eSTAR template requires that all subsections be completed, so if you are submitting a 510(k) to address a product change, you will want to include a justification for not including original information in required sections that did not change. Otherwise, all submitted information will be reviewed again, even if it does not differ from the original submission.
Review Timeline
The review timeline will be similar to the review timeline for a non-electronic submission for a 510(k). The guidance document “The 501(k) Program: Evaluating Substantial Equivalence in Premarket Notification [510(k)]” can offer more details. The same would apply for the De Novo in that you would need to reference the guidance document “De Novo Classification Process (Evaluation of Automatic Class III Designation)” for review timelines.
Tracking the Submission
The FDA secures the information about each submission’s progress so only its Official Correspondent (your company’s submission representative) can view it. You will be able to track the progress of your submission by using the Customer Collaboration Portal (CCP).
- If this is your Official Correspondent’s first time tracking a submission online, the FDA will automatically email a link to create a login password soon after the FDA starts its review.
- The FDA currently displays progress online for Traditional, Abbreviated, and Special 510(k) submissions.
- The FDA will formally notify you of your submission’s status by emailing your Official Correspondent with official actions and requests.
The future of eSTAR
These efforts are part of the FDA’s ongoing commitment to work with the industry and to improve the efficiency of the medical device review process. The final guidance for the 510(k) eSTAR was published this month and will become effective October 1, 2023, for 510(k) and De Novo submissions. In the long term if MUDUFA V is passed with the current requests from the FDA, the process will become a required standard for additional submission types such a PMA and will replace the need to mail eCopies containing eSTAR files through the FDA Collaboration Portal.

RAPS wrap-up
What a great conference! This year’s RAPS Convergence conference in Phoenix was outstanding by many measures. Not only was this the first time in quite a while that our community has had a chance to network in person, but our team also reported that the quality of conversations and presentations far surpassed their expectations. Kudos to the RAPS conference team for putting together a valuable and memorable experience.
We asked our team to share their thoughts about the conference, along with information they learned while attending sessions or in conversation with other RA professionals. We’ve compiled their thoughts below.
General thoughts on the conference
The consensus from our team was that this conference attracted a really good group of knowledgeable regulatory professionals and that the majority of sessions were incredibly informative. Everyone referenced great conversations they had throughout the conference.
.jpeg)
There were a lot of discussions around the challenges that RA teams face today, and what can be done to ease the burden of regulatory professionals in the face of ever-changing requirements across the globe.
I was impressed by the consistently high level of quality in the conversations I had. Every person I spoke with had an intimate understanding of the challenges currently faced by industry and expressed a willingness to engage in conversation about how to improve things. While there are clearly significant challenges to overcome, I am bullish about the future.
James Trotter
And regulatory teams are looking for ways to be less reactive and find time for strategic planning to prepare for future challenges.
One of my biggest takeaways is the true shift in thinking that is happening within the industry in regard to the need to think strategically about supporting regulatory teams. In a number of conversations, it was mentioned that RA folks wished that they had more time to take a step back and have future-facing conversations, rather than just “keeping up” with their day-to-day activities.
Alex Tallentire
We noticed how well-attended the sessions were and heard comments from a number of people that they were having trouble deciding which sessions to attend. RAPS has made presentation slide decks available to attendees through the conference website.
.jpeg)
Reggie, our regulatory duck, was also a big hit! Did you get one of our duck t-shirts?
Key session takeaways
CDRH Forum
The conversation was animated during the CDRH Forum, which ended with FDA stating “Communication is key. We take all feedback seriously and we are consistently making improvements.” Discussions centered largely around MDUFA V and the use of eSTAR templates. FDA is focusing on addressing the rising volumes of premarket submissions. This includes hiring additional reviewers, better support of 3rd party reviews to eliminate the need for FDA re-review, improved deficiency letter communication, and the expansion of electronic templates for submissions (including use with PMAs). They see these methods plus others as helping the agency meet the performance requirements on MDUFA V.
EU Regulations: PMCF and SSCP
Industry frustration - both by Notified Bodies and manufacturers - clearly continues over the burdensome requirements around PMCF and SSCP. As a subset of PMS, a PMCF plan is critical to MDR compliance and mandatory for Class III and implantable devices. Having a good plan is key, and industry is struggling to figure out what to do with the data once it is collected.
Because the audience for SSCP documents is healthcare professionals and patients, manufacturers will have to conduct readability assessments for each Summary of Safety and Clinical Performance (SSCP) through computer-based software programs or layperson assessments in all languages used in the EU market.
EUDAMED UDI
While the EUDAMED UDI module isn’t expected to be mandatory until the second quarter of 2026, there are triggering events that will require a manufacturer to enter data into the UDI module earlier. For example, mandatory use of the EUDAMED Vigilance module is Q4, 2024. If you have to report a product in the Vigilance module, that product must also be entered into the UDI module at that time. Bruce McKean, Rimsys Director of Regulatory, says that “Manufacturers cannot wait, they must be proactive rather than reactive when it comes to UDI.”
eSTAR
During the Solution Circle on “How to efficiently prepare your eSTAR submission,” attendees learned that FDA plans to expand the program to include more submission types. eSTAR submissions require a larger number of files attached to the PDF checklist, compared to the number of files submitted under traditional submission programs. One recommendation was to prepare your submission completely before filling out the eSTAR template. It seems apparent that the eSTAR program is designed to make the review process simpler for agency reviewers, but does not simplify the creation of the submission by the manufacturers.
If you are submitting a 510(k) to address a product change, the eSTAR template requires that all subsections be completed, even if they are not applicable to the change. This means that previously submitted and cleared information goes under review again. To avoid this, the recommendation was made that submitters include justification for not resubmitting data in these sections, rather than including the original data.
It is believed that the current guidance will be made final by the end of September 2022 with a one-year transition period for 510(k) and De Novo submissions.
What’s next?

RAPS has announced that next year’s conference will be in Montreal, October 3-5. We look forward to seeing everyone there (and we are working on next year's t-shirt design already). After this year’s great conference, we can’t wait to see next year’s!

FDA Class II medical devices
What are medical device classes within the FDA?
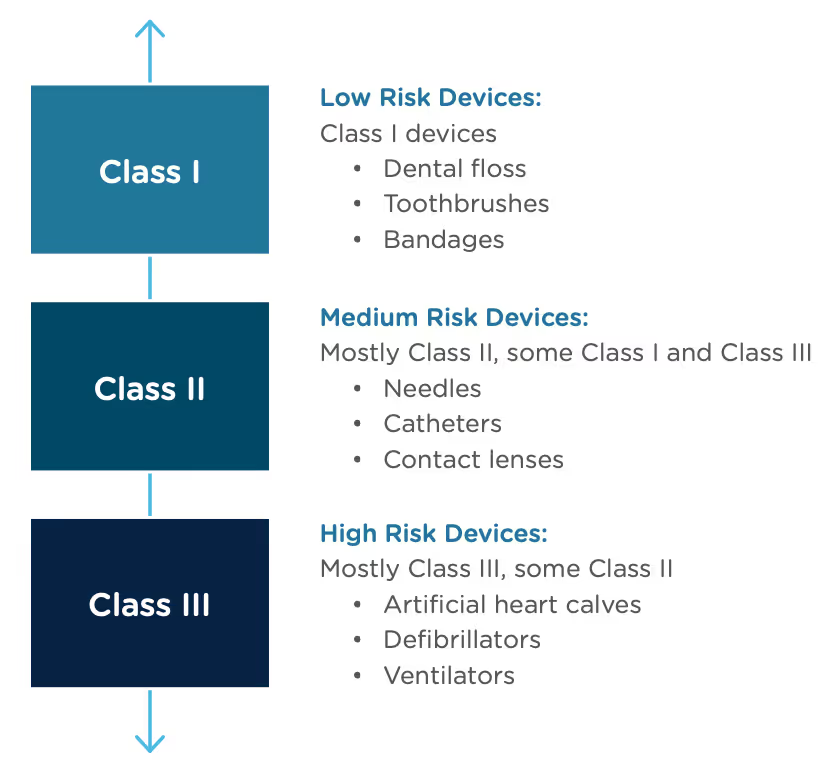
In the United States, the Food and Drug Administration (FDA) categorizes medical devices into three classes. They base these classes largely on the level of perceived risk the device may have. The level of perceived risk determines the data requirements and controls that need to be put into place to ensure safety for patients and/or users.
The FDA determines the level of oversight necessary for each device based on three factors. According to the FDA’s guidance on how to classify your device, device classification depends on the intended use of the device and also upon indications for use. The third and most important criterion is the device's risk to patients and users. The higher the risk associated with the device, the higher the class of that device will be, i.e Class I devices represent the lowest risk, and Class III devices pose the highest risk.
What are Class II Medical Devices?
Class II medical devices, which pose a medium to high risk to patients and users, account for 43 percent of all medical devices in the United States. Some common examples of Class II devices are syringes, pregnancy test kits, electric wheelchairs, and catheters. Class II medical devices must adhere to the provisions of the General Controls as mandated by the Food, Drug, and Cosmetic (FD&C) Act, which applies to all classes of devices.
The FDA also has its own Product Classification Database that can be used to assist in your device’s classification, finding consensus standards and submission types, such as a 510(k) or PMA.
What is the approval process for Class II Medical Devices?
All non-exempt Class II medical devices must go through the premarket notification process, also known as the 510(k). The 510(k) is a premarket submission process used to demonstrate that a device is safe and effective based on its substantial equivalence to a device already on the market, known as a predicate device.
Determining the substantial equivalence of your new device boils down to two things:
- Establishing that your device has the same intended use as the legally marketed predicate device
- Establishing that any technological differences between your device and the predicate device have no negative impact on the effectiveness and safety of the device
Any device with no identified predicate device, including those with a lower risk profile, is automatically classified as a Class III device and must use the more rigorous premarket approval (PMA) submission to receive market approval. Lower-risk devices can request reclassification, however, through a De Novo submission.
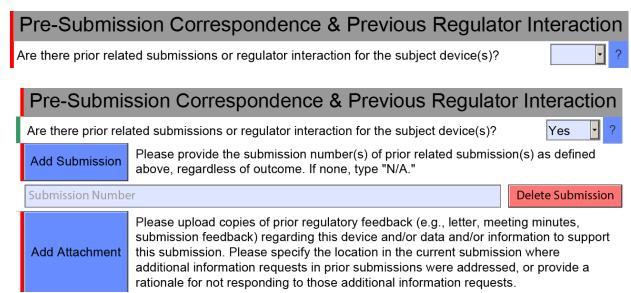
Class II medical devices in other countries
Device classification is different in each country. With that in mind, you should not make any assumptions regarding classification in other countries because your device is a Class II device in the United States. Each country with medical device regulations has its own classification scheme that may cause your device to be regulated differently.
During the initial phase of planning for the global commercialization of a product, it is imperative to consider international regulations, their classification schemes, and the registrations that each country will require.
The process of getting a Class II medical device to the market is arduous, and regulatory professionals must navigate disjointed manual data systems and processes. Plus, ever-evolving regulations make it difficult to ensure your new products, and even ones already on the market, are compliant.
Regulatory information management (RIM) software is an almost invaluable tool that can help your company get products to market more quickly and cost-effectively by digitizing and automating regulatory activities in a single system. The right RIM software can make the 510(k) process simpler and more efficient than ever before.
For more information on the 510(k) process, read our Beginner’s guide to the 510(k).
What's up with the duck?
If you’ve seen us online or at tradeshows, you might be wondering, “What’s up with the duck?” His name is Reggie by the way, and we’re pretty fond of him around here. Rimsys is more than software. It’s a team built from the ground up who understand the importance and challenge of managing regulatory affairs in the ever-evolving medical device industry. Our goal here at Rimsys is to help your company get its regulatory ducks in a row, and from that concept, “Reggie”, the regulatory duck was born.

If you could be a part of our company meetings, you’d see that we all love Reggie. After all, he’s more than a mascot to us. He symbolizes our mission to improve global health by accelerating delivery and increasing the availability of life-changing medical technologies. Reggie is our promise to our customers that you’re getting more than software with Rimsys. You’re getting a team of dedicated regulatory experts who understand the urgent need for better regulatory information and processes. That's why we love Reggie, our regulatory duck, and we believe you will too.
