


Featured
Rimsys Announces Rimsys AI to Eliminate Repetitive Tasks and Enhance Decision-Making for MedTech Regulatory Teams
Rimsys, the leading Regulatory Information Management (RIM) platform for the MedTech industry, today announced the launch of Rimsys AI, a suite of embedded artificial intelligence (AI) agents.

The beginner's guide to the FDA De Novo classification process
This article is an excerpt from The beginner's guide to the FDA De Novo classification process ebook.
Contents
- Introduction
- Chapter 1: What is an FDA De Novo request?
- Chapter 2: Contents of a De Novo request
- Chapter 3: Submitting a De Novo request
- Appendix A: Acceptance review checklist
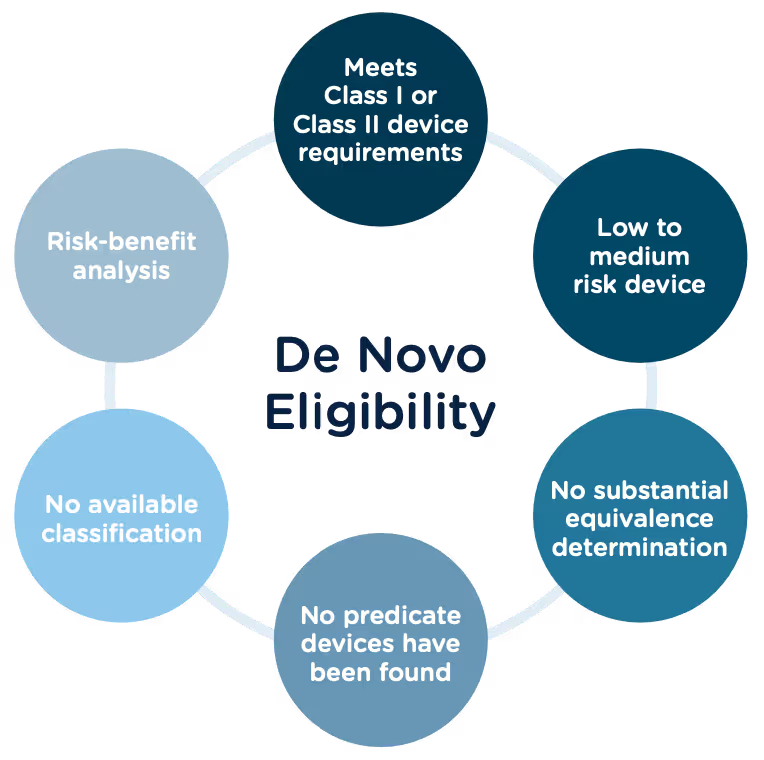
Congratulations, you have successfully developed a new medical device! Now you need to take it to market. Normally in the United States this would mean completing a 510(k) submission. However, the 510(k) relies on “substantial equivalence”—a comparison to a similar device already on the market (also called a predicate device) to assess the risk profile of the new device. What if your device is totally new, and there isn’t a similar device to compare it to? Enter the FDA De Novo process. The De Novo process provides a pathway to market for novel devices with a low to medium risk profile.
What does De Novo mean?
According to the Merriman-Webster dictionary, de novo is a Latin word meaning “as if for the first time; or anew.” Perfectly fitting that the FDA uses this term “De Novo” to describe market approval requests for new medical devices or technology where there is no comparable predicate device on the market.
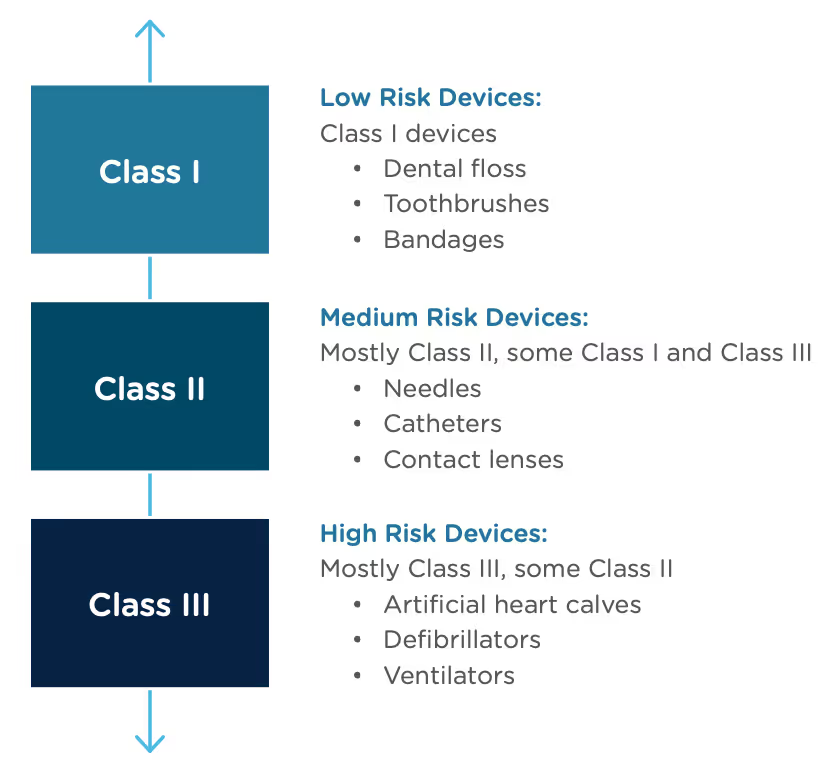
The Food and Drug Administration Modernization Act of 1996 provided the FDA with the authority to create the De Novo Classification Process. It's a process that uses a risk-based strategy for a new, novel kind of medical device, in vitro diagnostic, or medical software solution whose type has previously not been identified and/or classified. It’s a process by which a novel medical device can be classified as a Class I or Class II device, instead of being automatically classified as Class III, which may not be appropriate. Before the implementation of the De Novo process in 1997, all the “not substantially equivalent” (NSE) products were required to be initially classified as a Class III device. But for a lot of devices, this risk class didn’t really make sense. The De Novo process provides a pathway for more accurate classifications of novel, lower-risk devices.
October, 2021, the FDA released a final guidance document "De Novo Classification Process (Evaluation of Automatic Class III Designation)" to provide guidance to the requester (also known as the manufacturer) and the FDA on the process for the submission and review of a De Novo Classification Request under section 513(f)(2) of the Federal Food, Drug, and Cosmetic Act (the FD&C Act). This process provides a pathway to an initial Class I or Class II risk classification for medical devices for which general controls or general and special controls, provide a reasonable assurance of safety and effectiveness, but for which there is no legally marketed predicate device. This guidance document replaced the "New Section 513(f)(2) – Evaluation of Automatic Class III Designation, Guidance for Industry and CDRH Staff" document, dated February 19, 1998.
Consistent with the final rule, the FDA updated the guidance documents below to provide recommendations for submitting De Novo requests, as well as criteria and procedures for accepting, withdrawing, reviewing, and making decisions on De Novo requests, effective January 3, 2022.
- User Fees and Refunds for De Novo Classification Requests
- FDA and Industry Actions on De Novo Classification Requests: Effect on FDA Review clock and Goals
- Acceptance Review for De Novo Classification Requests
The 510(k) and the De Novo processes are similar in that they are both pathways to market for medical devices with low to moderate risk, which is Class I and Class II. The biggest difference between the two is that the 510(k) heavily relies on the concept of "substantial equivalence" to an existing medical device. You must prove this to get the clearance of your 510(k) submission. In the De Novo process, there isn’t a product currently on the market that is “substantially equivalent” to yours, so it’s like starting with a clean slate. For more on the 510(k) process, see our Beginner’s Guide to the 510(k) ebook.
A result of the De Novo process to be aware of is that a successful submission will lead to a new predicate device type that someone else can reference to bring their product to market through the 510(k) process. You’ve done all the work, so now it’s available for anyone to use to provide "substantial equivalence".
De Novo history/timeline
Preparing a De Novo request
1. Do your research! Be sure to complete all the necessary research prior to your submission. You want to be sure that your device is not substantially equivalent to an existing device. Resources to review include:
- The Center for Devices and Radiological Health (CDRH)
- U.S. FDA Device Classification Database
- Device Classification Under Section 513(f)(2)(De Novo)
2. A De Novo request can be submitted with or without a preceding 510(k). There are two options for when you can submit a De Novo request:
Option A: After receiving a not substantially equivalent (NSE) determination (that is, no predicate, new intended use, or different technological characteristics that raise different questions of safety and effectiveness) in response to a 510(k) submission.
Option B: If you’ve determined, after extensive research, that there is no legally marketed device on which to base a determination of substantial equivalence.
3. Be sure all fees are paid to the FDA in advance of submitting a De Novo request. The FDA’s fiscal year begins in October and runs through the following September. Fees have increased each year since they were introduced, but the FDA’s percentage of reviews completed within the 150-day window has increased as well.
A business that is qualified and certified as a “small business” is eligible for a substantial reduction in most of the FDA user fees, including De Novo. The CDRH is responsible for the Small Business Program that determines whether a business is qualified.
Medical Device User Fee Amendments (MDUFA) guidance documents can provide more detailed information about all FDA user fees.
4. The initial request process serves only to determine if the De Novo request is administratively acceptable based upon the Acceptance Checklist. The initial acceptance is followed by substantive review which will determine the final risk classification of your device.
5. A Pre-Submission (Pre-Sub) is a formal written request for feedback from the FDA that is provided in formal written form, and then followed by a meeting. Although a Pre-Sub is not required prior to a De Novo request, it can be extremely helpful to receive early feedback, especially for devices that have not previously been reviewed under a 510(k). If you think you would like to submit a pre-sub first, there are suggested guidelines for submission you should consider:
- Describe your rationale for a Class I or Class II classification for your device.
- Provide the search results of FDA public databases and other resources used to determine that no legally marketed device and no classification for the same device type exists.
- Provide a list of regulations and/or product codes that may be relevant.
- Provide a rationale for why the subject device does not fit within and/or is different from any identified classification regulations, based on available information.
- Identify each health risk associated with the device and the reason for each risk.
- Briefly describe any ongoing and/or planned protocols/studies that need to be completed in order to collect the necessary data to establish the device’s risk profile.
- Provide information regarding the safety and effectiveness of the device. Cite the types of valid scientific evidence you anticipate providing in your De Novo request, including types of data/studies relating to the device’s safety and effectiveness.
- Briefly describe any ongoing and/or planned protocols/studies that need to be completed to collect the necessary safety and effectiveness data.
- Provide protocols for non-clinical and clinical studies (if applicable), including how they will address the risks you anticipate and targeted performance levels that will demonstrate that general controls or general and special controls are sufficient to provide reasonable assurance of safety and effectiveness.
- Share any proposed mitigation measure(s)/control(s) for each risk, based on the best available information at the time of the submission. Highlight which mitigations are general controls and which are special controls and provide details on each.
- Include any other risks that may be applicable, in addition to those identified in the Pre-Sub, given the indications for use for the device.
- If applicable, provide any controls that should be considered to provide a reasonable assurance of safety and effectiveness for the device.
- Provide any non-clinical study protocols that are sufficient to allow the collection of data from which conclusions about device safety and/or effectiveness can be drawn. These protocols should address whether the identified level of concern is the appropriate level of concern for the device software, and if any additional biocompatibility and/or sterility testing is required.
- If clinical data is needed, provide information to show that the proposed study design and selected control groups are appropriate?
6. The FDA will attempt to review the De Novo request submission within 15 calendar days of receipt of the request to make a determination that the submission is declined or accepted for review. If they are unable to complete the review within the 15 days, your submission will automatically move to “accepted for review” status. https://www.fda.gov/regulatory-information/search-fda-guidance-documents/de-novo-classification-process-evaluation-automatic-class-iii-designation
7. There are times when the FDA will refund your application fee. They have created a guidance document “User Fees and Refunds for De Novo Classification Requests” for the purpose of identifying:
- the types of De Novo requests subject to user fees
- exceptions to user fees
- the actions that may result in refunds of user fees that have been paid
When is a De Novo request subject to a user fee?
When will the FDA refund a De Novo user fee?
What fee must be paid for a new device submission following a De Novo “decline” determination?
To continue reading this eBook including a detailed walk-through of all the Traditional 510(k) components, submission requirements and timelines, and an overview of the other 510(k) forms including the Abbreviated 510(k) and the Special 510(k), please register to download the full version.




An overview of the Accreditation Scheme for Conformity Assessment (ASCA) Program
Introduced in 2021, the Accreditation Scheme for Conformity Assessment (ASCA) program is a voluntary program that allows device manufacturers to use an ASCA-accredited testing laboratory to conduct testing to be included in premarket submissions to the FDA. The ASCA program is designed to speed up FDA review times, reduce guesswork on documentation to provide in a premarket submission, and improve the quality of testing conducted.
In September of 2023, the program was converted from a pilot to a permanent volunteer program. This blog post provides an overview of the ASCA program to help medtech companies determine if they should consider participating.
How the ASCA program works
Under the ASCA program, the FDA grants ASCA Recognition to qualified accreditation bodies, which certifies testing laboratories to perform premarket testing for medical device companies. The FDA uses international conformity assessment standards and FDA-identified ASCA program specifications to assess ASCA Accreditation status to qualified testing laboratories.
The ASCA program includes FDA-recognized consensus standards and related test methods across two scopes:
- Biocompatibility: This scope includes standards for testing the safety of medical devices when they come into contact with human tissues.
- Basic safety and essential performance: This scope includes standards for testing the safety and performance of medical devices.
It’s important to note that medical device manufacturers should continue to reference additional FDA-recognized standards and provide declarations of conformity in their premarket submissions, but standards outside of biocompatibility and basic safety and essential performance are not eligible for ASCA program benefits.
Medical device manufacturers can choose an ASCA-accredited laboratory to conduct its testing for FDA premarket submissions. The ASCA-accredited testing laboratory will provide the manufacturer with all information listed in the ASCA program specifications.
For each eligible FDA-recognized consensus standard and test method, the manufacturer will need to document results on an ASCA Summary Test Report. Upon testing completion, the device manufacturer will receive an ASCA Summary Test Report from the laboratory. When the manufacturer prepares their premarket submission for FDA approval, they will need to include a declaration of conformity with the ASCA Summary Test Report as part of their submission.
Benefits of participating in the ASCA program
Medical device companies that participate in the ASCA program can see a variety of benefits, including:
- Faster FDA review times: The FDA has stated that it expects to review premarket submissions that include ASCA Summary Test Reports more quickly than submissions that do not.
- More clarity on documentation needed in a premarket submission: The ASCA Summary Test Report template provides a guide on what information to include in the report, which can help device manufacturers avoid having to guess what the FDA is looking for. This can save time and resources and help to ensure that the premarket submission is complete and accurate.
- Improved quality of testing conducted: ASCA-accredited testing laboratories must meet rigorous standards for competence and impartiality.
- Enhanced credibility: Participating in the ASCA program can help device manufacturers enhance their credibility with the FDA and other stakeholders. This is because the ASCA program is designed to improve the quality and efficiency of the premarket review process.
While the FDA has not announced any plans to make the ASCA program mandatory, it has stated that it intends to review premarket submissions that include an ASCA Test Summary report faster. This means that device manufacturers who participate in the ASCA program may be more likely to receive faster approvals.
In addition, some countries outside of the United States require device manufacturers to use accredited testing laboratories for premarket approval. By participating in the ASCA program, device manufacturers can demonstrate that their testing is conducted to high standards and more easily meet the requirements of these countries.
Funded through the MDUFA V User Fee program, the FDA does not charge an additional fee for manufacturers to participate in the ASCA program. For more guidance and training on the ASCA program, see the FDA’s website.

Your eSTAR submission questions answered by FDA experts
Your eSTAR submission questions answered
Starting on October 1, 2023, all 510(k) submissions, unless exempted, will need to be submitted electronically using eSTAR. eSTAR, which is short for Electronic Submission Template and Resource, is a dynamic PDF submission template that contains automation, guides, integrated databases, integrated policies and procedures, and automatic verification to help users prepare a comprehensive medical device submission.
Rimsys recently hosted a webinar, eSTAR submissions overview and live Q&A with FDA, to help the medtech community prepare for the quickly approaching eSTAR deadline. Patrick Axtell, Assistant Director for Tools and Templates Team, and Sajjad Syed, Software Engineer for Tools and Templates Team, from FDA joined our panel of Rimsys regulatory experts to provide an overview of eSTAR, demo, and live question and answer session. If you're interested in watching the webinar replay, you can find it here.
Due to high participation, we couldn't answer all questions live. This blog post provides Patrick's and Sajjad's answers to questions we couldn't get to during the webinar. Read below to learn what other industry professionals want to know about eSTAR!
Q: In the past, the sections were numbered Section 10 - Device Description. How should section(s) be numbered in the eSTAR?
You may number attachments how you prefer, this includes numbering attachments according to the previous section numbers of the Format for Traditional and Abbreviated guidance document. However, the numbering hierarchy in the IMDRF documents, which the attachment questions in eSTAR correlate to, may be better, since that numbering scheme is internationally harmonized. So for example, if you are using the nIVD eSTAR, the IMDRF document specifies the Comprehensive Device Description would be numbered 2.04.01: https://www.imdrf.org/sites/default/files/docs/imdrf/final/technical/imdrf-tech-190321-nivd-dma-toc-n9.pdf.
Q: After October 1, 2023, will the In Vitro Diagnostics eSTAR Version be acceptable to use for a Dual 510(k) and CLIA Waiver by Application (Dual Submission)?
Yes, the next IVD eSTAR update will fully support Dual submissions, and the workaround we were previously implementing will no longer be needed. CLIA waiver submissions will continue to be submitted via current methods, and are not required to use eSTAR after Oct 1, 2023.
Q. It is not possible to view eSTAR online from cloud storage platforms. eSTAR like IFU Form and CDRH Form cannot be viewed online without users downloading these files. I will highly appreciate if someone from the panel can give a solution to this. I understand these are special pre-programmed PDFs but it will immensely help if these can be shared for online viewing without having users download these files.
You need to choose to open eSTAR in the default application from within the cloud application you use, you can’t just click on it, since it will open in the browser, and browsers can’t open dynamic PDFs like eSTAR, Form 3881, Form 3514, and other forms FDA uses.
We can’t say that all cloud applications will work, but using Box does work. Once eSTAR is loaded in, click on the three dots, then choose the application you have installed, see screenshots below. I have Adobe Acrobat 2017 and Adobe Acrobat Pro both installed.
Be aware that every time you save the form, you upload it back into the cloud, so depending on how large it is and how fast your internet connection is, it may take many seconds to save each time, though you will see a progress bar.
Q: Does the eSTAR submission need to be submitted by only the US Agent or can this be done by the Foreign Manufacturer?
510(k) eSTARs, like 510(k) eCopies, can be submitted by foreign applicants.
Q: Will it be mandatory to use the eStar template for PMA supplement submissions?
Yes, by the end of 2023, eSTAR for PMA will be released. Similar to eSTAR for 510(k), there will be a pilot, guidance, and a transition period before it becomes mandatory.
Q: When do you expect to release the next version or sub-version of the non-IVD eSTAR template (4.x or 5.0) and will it be more elaborate on cybersecurity?
We are at the mercy of updating when policies are updated, which is irregular and unpredictable. Please email CDRH management and recommend a more consistent (e.g. quarterly) policy deployment schedule so that eSTAR can also have a more predictable deployment schedule. We are updating approximately one to every two months currently. Please be sure to read the Version History on page 1 of eSTAR regarding versioning and which version to use.
Q: How should a device categorized as a breathing gas pathway device in accordance with ISO 18562 be handled in eSTAR? One cannot find ISO 18562 categorization for a device in the eSTAR form.
This is a regulatory and policy question, and we are not sure what is meant by the statement “be handled.” Please reach out to OPEQ Submission Support OPEQSubmissionSupport@fda.hhs.gov with this question and they will direct your question appropriately.
Q: How often does FDA anticipate revising the eSTAR form?
eSTAR updates are almost exclusively timed according to policy updates, which the Tools and Templates Team has no control over. The T&T Team, as well as other groups in CDRH, are pushing for a quarterly update, where any policy updates in a quarter have an implementation date set for the beginning of the next quarter (e.g. Oct 1st, Jan 1st, Apr 1st). Please email Center management and promote this.
Q: The guidance Format for Traditional and Abbreviated 510(k)s: Guidance for Industry and FDA staff recommends a specific format for submissions. Biocompatibility, for example, is section 15. Should attachments in the eSTAR submission cross-reference the sections cited in the guidance? (So still using biocompatibility as an example, attachment 15.1 would be Cytotoxicity, attachment 15.2 would be Sensitization and so on)
The Format guidance, as well as the eCopy guidance, RTA guidance, and many other guidances, no longer apply for eSTARs. Eliminating the applicability of guidances - simplifying the preparation process - is something we are proud of doing. You do not need to follow the numbering of this guidance. See response above, where we recommend using the IMDRF numbering scheme instead, which is internationally harmonized.
Q: Where is information for risk assessments and management best included?
Depending on the type of submission you have selected (e.g. 510(k), De Novo, then Traditional, Special, Abbreviated), certain sections will become visible and active and some of them will be disabled. However, the bookmark pane will show all the sections in the entire eSTAR. Hence, please fill the sections that are visible to you since they are based on your selections. For example, if you have selected a Traditional 510k, the “Benefits, Risks and Mitigation Measures” section is not applicable. Hence it is not displayed and clicking on it leads a user back to the first page of the eSTAR. However, if you select “Special” as the 510k you are submitting, the “Benefits, Risks and Mitigation Measures” section does become applicable, and is displayed if you click on the bookmark. Also note that if you select De Novo, the section does become active as well. Another point to note is that for a Traditional 510(k) submission, if you do want to submit a Risks, Mitigations, Benefits report, you can attach it in the Performance Testing --> Bench Testing section of the eSTAR and identify it as “Other Non-Clinical Evidence”.
Q: Under Biocompatibility any idea when there will be endpoint questions for hemocompatibility or coagulation?
Hemocompatibility endpoint information, including Hemolysis, Complement Activation, and Thrombogenicity information, will appear depending on the tissue contact type and duration you choose. If you choose Implant Device >30 days, you will see this tab appear for example. The tabs that show are based on our Biocompatibility guidance.
Q: Guidance and Special Controls Adherence Section: According to the 510(k) electronic submission guidance document, identification of any applicable device-specific guidance documents or special controls should be included, which was done in the past; however, eSTAR requires each specific special control regulation or guidance recommendation to be listed. Can you please specify to what level of detail needs to be included within this section? The text box contains a character limitation, so it is unclear how specific information needs to be.
There are four textboxes like this in eSTAR. The specifications, characteristics, etc., of the device should not be provided in these textboxes. Instead, these textboxes should be used to refer to the attachments where these controls or recommendations are found, per each specific recommendation. These textboxes do expand as text is typed in, if needed. Keep in mind that the special controls, device-specific guidance citations would be divided among these four textboxes.
Q: Why are Advertisements included within the Labeling section, when they should be considered promotional materials? Could reference to advertisements be removed from this section?
Advertisements and promotional materials are included under the Other Labeling, and within the sub-attachment type "Other Labeling and promotional material" since this is consistent with Internationally harmonized document N9 and N13. As the help text states, whether you actually need to attach it at all (it is an optional attachment) is dependent on the jurisdiction. For FDA, you would need to reach out regarding your device and current policy at opeqsubmissionsupport@fda.hhs.gov.
Q: I need to know how eSTAR would promote efficiency.
There are many efficiency gains with eSTAR, this is not an exhaustive list. The eSTAR website also includes some of this information.
-eSTAR complements the reviewer's internal smart review template used to review the submission (i.e. the questions correlate). Therefore the reviewer is getting what they are expecting
-eSTAR provides a standardized format so that the reviewer (and applicant) always know where to find certain information
-eSTAR auto-updates many aspects of the submission, most notably it ensures the content is present negating the need for an RTA review by the reviewer, and therefore RTA holds
-eSTAR autocompletes information that you enter, ensuring you never need to enter the same information twice
-eSTAR includes built-in databases that ensure you see the information pertinent to your device (e.g. device-specific guidances), classification information automation, and the standards database, for auto-filling standards info accurately
-eSTAR has many forms built in, so that you don’t need to attach or upload them (e.g. T&A statement, Form 3514, 510(k) Summary, Declaration of Conformity, Form 3881)
-eSTAR guides the applicant through what is needed throughout, ensuring we collect everything that needs to be provided, and you know how to do it correctly
-eSTAR is collecting submission data in a structured format, which will help automate many aspects of our processing. This will provide applicants and reviewers many benefits (e.g. automating the submission log-in process, therefore permitting reviewers to receive a submission within minutes of when the submission is uploaded in the CDRH Portal)
-eSTAR is intended to be used as a resource also, since it consolidates all the information needed (e.g., regulation links, guidance links, submission process information) to prepare a submission

Rimsys ranks number 156 on the 2023 Inc. 5000
Rimsys is happy to announce today that it has been ranked number 156 on the 2023 Inc. 5000 list of fastest-growing private companies in America. Companies on the 2023 Inc. 5000 are ranked by their percentage of revenue growth over a three-year period. With exponential growth over the past three years, Rimsys joins a prestigious list of organizations across the country.
Rimsys, a cloud-based software for end-to-end regulatory process digitization and automation, is designed by and for medtech regulatory affairs professionals who experienced the painful challenges and compliance risks that result from not having a centralized, collaborative hub for regulatory information.
"Being included on this year's Inc. 5000 list of fastest-growing private companies is a tremendous milestone for Rimsys," said James Gianoutsos, Founder and CEO. "I created Rimsys to help medical device manufacturers overcome the challenges I experienced in the industry, and our regulatory information management (RIM) platform has increasingly gained the trust of leading medical device manufacturers globally over the past few years. I'm excited to continue our mission of improving global health by accelerating delivery and increasing availability of life-changing medical technologies with the support of our team members, customers, and partners."
The top 500 companies, including Rimsys, are featured in the September issue of Inc. Magazine, which will be available beginning August 23. To see the complete results of the Inc. 5000, view company profiles, and access an interactive database of honorees, visit www.inc.com/inc5000.
About Rimsys
Rimsys is improving global health by accelerating delivery and increasing availability of life-changing medical technologies. Rimsys Regulatory Information Management (RIM) software digitizes and automates regulatory activities, helping medtech regulatory affairs teams to plan more effectively, execute more quickly, and confidently ensure global regulatory compliance. Unlike complex, color-coded spreadsheets, or expensive external consultants, Rimsys centralizes all regulatory information, automates submission processes, and provides detailed visibility into product registrations, expirations, relevant standards, and global regulations. Traditional approaches to regulatory affairs can’t keep pace with the growing complexity of the global landscape, and overburdened teams face increasing compliance risks. Rimsys is designed around medtech regulations and workflows and supports a full breadth of regulatory activities including registrations, submissions, UDI, essential principles, standards management, and regulatory intelligence in a single, integrated platform. Leading global medtech companies including Johnson & Johnson, Siemens Healthineers, and Omron rely on Rimsys to better manage regulatory projects and resources, get new products to market more quickly, and reduce revenue risk of non-compliance, product recalls, and unexpected expirations. For more information, visit www.rimsys.io.
About Inc.
Inc. Business Media is the leading multimedia brand for entrepreneurs. Through its journalism, Inc. aims to inform, educate, and elevate the profile of our community: the risk-takers, the innovators, and the ultra-driven go-getters who are creating our future. Inc.’s award-winning work reaches more than 50 million people across a variety of channels, including events, print, digital, video, podcasts, newsletters, and social media. Its proprietary Inc. 5000 list, produced every year since 1982, analyzes company data to rank the fastest-growing privately held businesses in the United States. The recognition that comes with inclusion on this and other prestigious Inc. lists, such as Female Founders and Power Partners, gives the founders of top businesses the opportunity to engage with an exclusive community of their peers, and credibility that helps them drive sales and recruit talent. For more information, visit www.inc.com.

An overview of the Medical Device Discovery Appraisal Program (MDDAP)
Regulatory affairs within the medtech industry is uniquely challenging. Teams are faced with external changes in the form of new regulations (such as the MDR/IVDR in the European Union), growing information needs (including expanding unique device identification requirements around the world), newer audit requirements (MDSAP), and post-market surveillance requirements.
While there are emerging technologies that can help teams better address these issues, building more effective and efficient regulatory teams requires more than better tools. The traditional, largely manual approach to regulatory procedures and processes must also evolve, including the measurement of regulatory maturity. The Medical Device Discovery Appraisal Program (MDDAP) was born out of the recognition that regulatory compliance does not, by itself, guarantee the highest quality devices and was designed to enable device makers to measure their capability to produce high-quality devices.
This blog post provides a high-level overview of the Medical Device Discovery Appraisal Program (MDDAP) to help organizations assess the benefits of participating.
What is the Medical Device Discovery Appraisal Program (MDDAP)?
MDDAP provides the model for the Case for Quality Voluntary Improvement Program, a collaborative program between the FDA Center for Devices and Radiological Health (CDRH), the Medical Device Innovation Consortium (MDIC), Information Systems Audit and Control Association (ISACA), and the medical device industry. The Case for Quality program was initially started by the FDA in 2011 to identify manufacturers that consistently produce high-quality devices along with the practices that have the greatest impact on quality.
A timeline of MDDAP:
- 2011 – FDA launches Case for Quality
- 2018 – FDA and the Medical Device Innovation Consortium (MDIC) implement a voluntary pilot program for medical device manufacturing sites using the key business process and best practices detailed in the ISACA Capability Maturity Model Integration (CMMI) system
- 2022 – On May 5, 2022 the FDA issued the draft guidance, Fostering Medical Device Improvement: FDA Activities and Engagement with the Voluntary Improvement Program.
The draft guidance issued in May, 2022 outlines the transition from the pilot program to a permanent program, titled the Case for Quality Voluntary Improvement Program. The Voluntary Improvement Program (VIP) is facilitated through the Medical Device Innovation Consortium (MDIC) which will utilize the Capability Maturity Model Integration (CMMI) to evaluate the capability and performance of the participating medical device manufacturers. Originally developed to optimize an organization’s software development process, CMMI is now used in many industries to provide a methodology and assessment tools for continuous improvement.
The MDDAP program is voluntary and leverages the CMMI model to provide medical device manufacturers, who are already in compliance with FDA quality and regulatory requirements, with insight into how they perform against selected best practices. The program is designed to help already-compliant organizations identify gaps in existing processes and increase the ability to react to change and avoid previously unforeseen quality and process issues.
Requirements for MDDAP participation
Any facility which “designs, manufacturers, fabricates, assembles, or processes a finished device” in the United States is eligible for participation, with the following additional requirements:
- The organization must have a prior compliance history or compliance profile through an FDA inspection or MDSAP audit.
- The participating site must be registered with the FDA.
- The device must be listed with the FDA.
- The organization cannot currently be under an Official Action Indicated (OAI) or subject to judicial action.
Participants in the program can include those with Class I, II, or III devices and, in addition to being device manufacturers, may also perform contract sterilization, relabeling, remanufacturing, repacking, or specification development.
Visit the ISACA MDDAP site to see if your organization qualifies.
Advantages for manufacturers participating in MDDAP
The MDDAP program provides operational advantages by streamlining multiple regulatory processes with the FDA, as well as longer-term benefits to product quality and organizational processes. The program is built on the CMMI framework which identifies processes most effective in decreasing risk and improving product quality.
MDDAP participants who have completed appraisals through the program will have the following advantages when working with the FDA:
1. Reduced inspection activities - A risk-based approach to FDA inspections allows manufacturers to bypass routine FDA surveillance audits and PMA preapproval inspections for participating sites. The participating site will have demonstrated compliance with the quality system regulations verified by FDA through inspection (a prerequisite for joining the program). MDDAP appraisals and quarterly checkpoints evaluate the participating organization against a proven set of best practices and provide guidance on continuous improvement projects.
Participants should understand that the FDA will still perform “for cause” or directed inspections as required based on safety signals or as a follow-up to a safety event. Also, note that organizations participating in the MDSAP program will still need MDSAP audits.
2. Streamlined change notices - Participants in the MDDAP program have access to modified submission formats for:
- PMA and HDE 30-day change notices. Resources permitting, the FDA intends to review changes within the reduced timeframe of 14 calendar days.
- PMA and HDE manufacturing site change supplements.
- PMA or HDE manufacturing modules.
3. A more collaborative process with the FDA - The FDA’s Case for Quality program was designed to provide a more collaborative approach to medical device compliance and quality. This differs from the traditional oversight models by going beyond regulatory compliance and focusing on continuous improvement projects that optimize device quality.
Perhaps the biggest benefit of participating in the MDDAP program, however, is that the program provides a methodology for evaluating an organization's “maturity level” and implementing continuous improvements toward the goal of optimizing quality. Participating organizations are committing to a proven continuous improvement program. This results in the ability to consistently ensure a high-level of quality that can yield significant competitive and market advantages.
Are you looking for more tips to help your regulatory team achieve competitive advantages? Read our ebook, Regulatory strategy as a competitive advantage.

Competent Authority, Notified Body, Authorized Representative – who’s who and what do they do?
Marketing medical devices in the European Economic Area (EEA) can be a challenge as manufacturers must navigate changing regulations, and an array of agencies across the region and in specific countries. Some regulatory activities require interactions with regional level authorities, while others are handled by Member States, and it’s not always clear when to engage with which authority.
This article explains the different regulatory bodies that oversee medtech products within the European region, their roles in the market clearance processes, and a full list of relevant country-specific authorities.
Competent Authorities
A Competent Authority belongs to the government of a Member State of the European Union (EU) and is responsible for transposing the requirements of European regulations into national legislation. There is an umbrella group called the Competent Authorities for Medical Devices (CAMD) that is responsible for improving communication and collaborative work between these competent authorities, and increasing the surveillance of medical devices on the market. All of the competent authorities work together in the CAMD network to support patient safety and organize the implementation and the enforcement of the regulations on medical devices and in vitro diagnostic devices.
Notified Bodies
Medical devices are initially reviewed and approved by a Notified Body before they are placed on the market. Notified Bodies are supervised by the Competent Authority of a particular EU Member State. A Notified Body is an independent organization designated by an EU Member State to make sure that the Medical Device Requirements (MDR) and In Vitro Diagnostic Requirements (IVDR) are being followed for as long as the product remains on the market. Notified Bodies are also designated for specific directives, regulations, or products that need higher and stricter safety standards, or those that weren’t built according to harmonized EN standards, such as electronic equipment, gas appliances, and certain medical devices.
A medical device that has been approved for the market will bear a “CE mark” which indicates that it meets the basic requirements for safety and effectiveness under European law. In addition, The Commission assigns a 4-digit code to each Notified Body, with the purpose of uniquely identifying each company that acts as a Notified Body. The codes range from 0001-2900, and they must be placed below the CE Mark on the product and/or it’s packaging, and on the user manual.
Authorized Representatives
According to EU directive 2017/745 and 2017/746, it is a legal requirement to appoint a European Authorized Representative (EU Rep) for a medical device manufacturer who does not have a registered place of business in a particular EU Member State. This role will be the liaison between the manufacturer and the Competent Authority. The name and address of the EU Rep must be included on the labelling, outer packaging or on the instructions for use as designated in EN ISO 15223-1:2021
Generally speaking, each Member States’ Competent Authority is responsible for monitoring the safety of medical devices after they are placed on the European market. They are given the authority to act on behalf of the government of an individual European Union Member State to ensure that the regulations are being monitored for compliance with the national statutes and regulations according to EU law.
EU National Competent Authorities
A list of contact points for each of the authorities can be found on the European Union website.
Managing regulatory complexity for European submissions and compliance
Deciphering agencies, and understanding when to engage with which authorities is only one of the complexities that medtech regulatory affairs professionals have to deal with. The new MDR and IVDR regulations have introduced new product registration, universal unique device identification (UDI), and standards and evidence requirements. At Rimsys, we’ve authored several ebooks to help regulatory affairs teams navigate these changes. For more information, check out:

Selecting and working with medtech regulatory approval consultants
Medical device organizations often use consultants to assist with regulatory approval projects. Regulatory consultants, however, have a wide variety of experiences and capabilities, and can add value to many types of regulatory projects. It is important to find a consultant that not only has the expertise to work on the project you need assistance with, but is also the right match for your team and your organization.
Selection criteria
Using a combination of referrals and research, you should be able to develop a short list of consultants that you would like to further evaluate. Consultants that have worked on similar projects or with similar organizations should be at the top of your list. Before you finalize that short list, however, and as you prepare to talk to consultants about potentially engaging with your organization, put together a requirements list that includes your needs in the following areas.
- Experience with similar organizations - The more closely a consultant’s specific experience matches your organization, the more quickly they will be able to add value to your project. Ask how much experience they have working with organizations your size and in your country, as well as experience in the countries in which you are marketing products.
- Regulatory expertise – The type of project will dictate the specific regulatory expertise your consultant needs. For example, are you looking for a consultant with experience bringing a product to market in a specific country, experience addressing a particular quality issue, or expertise with a particular RIM or eQMS system?
- Size and scope - Regulatory consultants vary in size ranging from large, international organizations to smaller firms to single, independent consultants. There are advantages and disadvantages to working with consultants in each of these categories. For example, a large organization will be able to provide a wide range of services and experts but may come with higher administrative costs and hourly rates. Smaller consulting firms can often offer a more tailored and flexible approach.
- Cost – When discussing costs, be sure to look at the expected overall project cost. While larger firms may have higher average hourly rates, they may also provide less-experienced consultants for some project tasks. Smaller firms may offer more flexible payment terms and be more willing to negotiate rates and fees.
- Communication style – Discuss the methods and timing for communication with the consultant and ensure that they match your expectations.
To ensure a good match between your organization and a regulatory consultant, evaluate team capabilities and discuss any additional expectations you will have for the consultant with your executive sponsors and management team. Ultimately, the best way to ensure a good match is to talk with other organizations that have used the consultant for similar projects.
Contractors vs Consultants
Contractors are similar to consultants but are more often used to fill the gap between the resources you have and the resources you need to stay on top of all regulatory activities within your organization. Contractors perform work that is assigned to them and they are not typically expected to manage projects, while consultants are most often hired on a project basis and are expected to bring their unique expertise to your project.
Getting the most out of the relationship with your regulatory consultant
Your organization will benefit more from a consultant if you actively manage the relationship by:
- Taking advantage of the consultant’s expertise – Don't miss the opportunity to learn from your consultant and consider giving them some leeway to point out issues they see that might be beyond the scope of the existing project.
- Maximizing your consultant's time – Clearly identify expectations with the consultant to ensure that they are spending time where they can add the most value and help you achieve the project’s goals as quickly as possible.
- Timing your consulting engagements – In many cases, a good regulatory consultant will be able to provide the greatest value when they work with you from the start of the project.
- Resources for the consultant – Regulatory consultants will need access to data, information, and systems - appropriate to their work on your project. Establishing access ahead of time can provide a smoother transition for the consultant and ensures that proper security procedures are followed.
Engagement types
The project scope and objectives will help you to define the type of consultant engagement. Types of consulting agreements include:
- Fixed projects – Fixed projects may be billed hourly or on a project basis, but typically have built-in payment milestones. Fixed projects will have a specific end goal that is easily defined and measured.
- Advisory engagements – Also referred to as “open-ended” agreements, advisory engagements allow you to access consultant resources and expertise on an as-needed basis. While somewhat open, these types of engagements should include caps on cost and an end date.
- Resource augmentation – When your regulatory team isn’t large enough to handle the current workload, consultants or contractors can be used to augment your existing capabilities. These agreements are usually very specific in terms of the services provided and you should still carefully define the consultant’s role and scope of work.
If you are working with a regulatory consultant on a RIM selection project, read more about selecting a RIM system for your medical device company.
