


Featured
Rimsys Announces Rimsys AI to Eliminate Repetitive Tasks and Enhance Decision-Making for MedTech Regulatory Teams
Rimsys, the leading Regulatory Information Management (RIM) platform for the MedTech industry, today announced the launch of Rimsys AI, a suite of embedded artificial intelligence (AI) agents.
.avif)
2023 Regulatory performance report
Today at Rimsys, we unveiled the 2023 MedTech Regulatory Performance Report, a new set of insights into the state of medtech regulatory affairs. Compiled based on interviews with 200 regulatory professionals and executives, the study provides a detailed look into how regulatory teams are staffed, their processes, the tools they use, and ultimately how they perform.
Why did we create this study? There were two driving factors behind the research. The first was a common theme that we heard from a number of our customers: Regulatory leaders don’t have clear data and benchmarks. They don’t necessarily know how long a new market submission should take, and how to plan for or assess the work of their teams. While other studies look at the medtech industry broadly or the state of the regulatory profession, this study tries to build a comprehensive resource for regulatory (and company) leaders.
The second factor was really for ourselves and the team at Rimsys. As a company building solutions specifically for medtech regulatory affairs, we wanted more insight into where companies were successful, where they struggled, and where we can add value.
What did we find? Regulatory teams perform a lot of hero work and rate themselves highly for their accomplishments. At the same time there is a lot of opportunity for process improvements, and companies that invest in digital transformation for regulatory affairs see better performance.
Regulatory professionals are superheroes
Regulatory teams are generally pretty small. Most companies have less than 10 full-time regulatory professionals. These small teams complete an enormous amount of work. Last year on average, RA teams completed 50 license renewals, 50 license updates, and 10 new market submissions. This is impressive output.
Digging a bit under the covers, we found that this output relied heavily on the support of external consultants. 90% of companies use consultants to keep pace with their regulatory workload. Front-line employees also struggle with burnout. They were much more likely to report feeling under-resourced than regulatory leaders.
But process problems persist
A lot of regulatory work remains extremely manual. 70% of regulatory teams spend half their time or more on repetitive administrative tasks. All of this manual work increases the frequency of errors and required rework. 61% of companies reported a major non-compliance incident in the past 2 years.
Manual work also makes it difficult to complete regulatory projects in a timely fashion. Teams completed a lot of projects, but each took a long time. Over half of all companies spend 4 months or more on license renewals, license updates, and new market submissions.
Moving regulatory affairs forward
As regulatory requirements become more complex, there’s a natural question about how teams will work moving forward. MDR & IVDR in Europe have significantly increased the regulatory workload required to bring and keep products on the market. Will organizations be able to keep pace with the same resources, tools, and processes?
No, and the performance report shows that medtech companies are investing to improve their regulatory capabilities. The majority of companies are planning to increase the sizes of their RA teams in 2023, and 40% expect to increase their investments in regulatory software. Companies are increasingly adopting specialized software to better support regulatory processes.
Dig into the survey results
The full survey results provide insights into more aspects of regulatory performance. They show that companies need to take a deeper look into their processes and how regulatory resources are allocated. There are two ways to learn more:
- Visit the survey page to see the full results (the survey whitepaper can be downloaded at no cost)
- Watch the recording of our webinar with PA Consulting. We discuss the survey results in more detail and share our regulatory predictions for 2023


Post-market surveillance for medical devices in the European Union
This article is an excerpt from Post-market surveillance for medical device in the European Union.
Table of Contents
- What is post-market surveillance?
- What classes of medical devices require post-market surveillance?
- Components of a successful post-market surveillance plan
- PMS data requirements
- Post-market surveillance system goals
- Required post-market surveillance reporting
- Embracing post-market surveillance as an integral part of your quality program
- Getting started with post-market surveillance
Post-market surveillance (PMS) is designed to monitor the performance of a marketed medical device by collecting and analyzing field use data. Article 10 of the EU MDR and IVDR requires all device manufacturers to have a post-market surveillance system in place. The main elements of the PMS are laid out in Article 83, and additional details for lower-risk and higher-risk devices are covered in articles 84 and85, respectively.
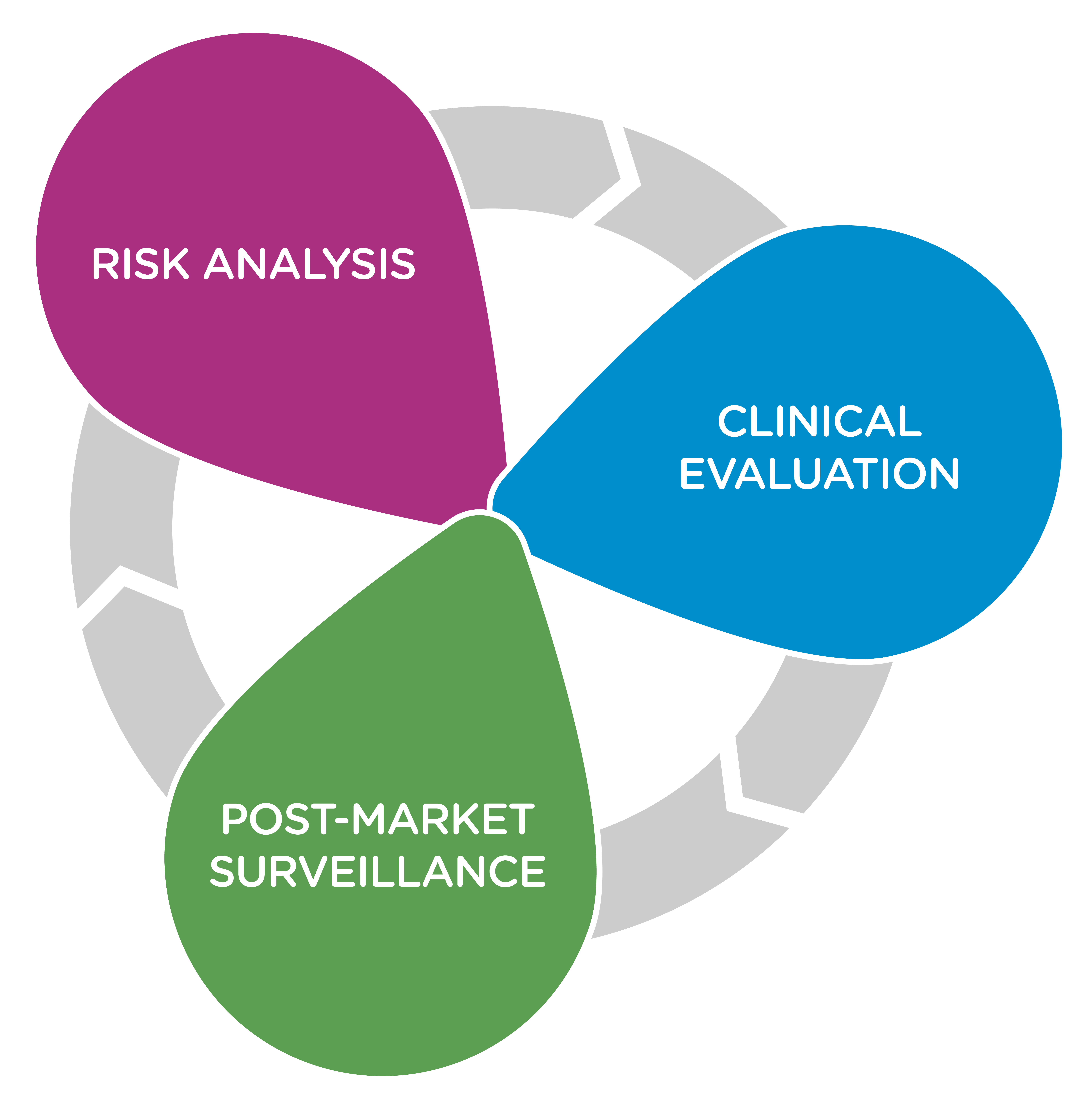
In general, a PMS system consists of both proactive activities and reactive, or vigilance, activities. While post-market surveillance and vigilance are sometimes used interchangeably, vigilance consists of separate activities that feed post-market surveillance programs.
Post-market surveillance systems are used to collect and analyze data not only about the manufacturer’s device but also about related competitors’ devices that are on the market. Data collected through PMS procedures is then used to identify trends that may lead to, among other things, quality improvements, updates to user training and instructions for use, and identification of manufacturing issues.
Note that “market surveillance” encompasses activities performed by a Competent Authority to verify MDR compliance, and should not be confused with the topic of this ebook,“post-market surveillance," which is performed by the manufacturer.
All medical devices marketed in the EU require some level of post-market surveillance, and all medical device manufacturers must implement a post-market surveillance system (PMS). The requirements of the PMS, however, vary and should be “proportionate to the risk class and appropriate for the type of device” (MDR Chapter VII). In particular, the type and frequency of reporting vary based on a device’s risk class.
A post-market surveillance plan (PMS) is an integral part of a manufacturer’s quality management system and provides a system for compiling and analyzing data that is relevant to product quality, performance, and safety throughout the entire lifetime of a device. The PMS should also provide methods for determining the need for and implementing any preventative and corrective actions. A PMS system should include and define:
Surveillance data sources
With the increased focus on proactive risk identification in the MDR, it is important to design post-market surveillance systems that actively acquire knowledge and detect potential risks. It is not sufficient to rely solely on spontaneous reporting by healthcare providers, patients, and other stakeholders.
In addition to information coming from Clinical Evaluation Reports and complaint and adverse event reporting, typical sources of surveillance data include:
• Social media networks: Because many of your stakeholders may be communicating on social media networks, it is important to employ social listening techniques and/or tools to identify issues and concerning trends as they develop.
• Industry and academic literature: Any studies, academic papers, and other literature that addresses similar devices or the specific use cases for which your device is designed should be evaluated. In particular, risk factors and adverse events identified with similar devices should be closely examined. It is also important to identify newer technologies that may affect the benefit-risk ratio and establish a new definition of “state of the art” for the device type.
• EUDAMED: While the European Database on Medical Devices (EUDAMED) is not yet fully functional, it is intended to provide a living picture of the lifecycle of all medical devices marketed in the EU. Manufacturers should take special care to consider information for similar devices made available through the EUDAMED system in the future.
• Registries: Patient, disease, and device registries can provide information that informs the clinical evaluation process which provides input into the post-market surveillance system.
Data analysis methodology
A well-defined data analysis methodology will accurately identify trends and lead to defendable decisions in the application of post-market experience. Once the necessary information has been identified and collected, and potentially cleaned of incomplete or otherwise unusable data, the data needs to be analyzed.
The goal is to identify meaningful trends, correlations, variations, and patterns that can lead to improvements in the safety and efficacy of the device. There are many data analysis tools available that can assist with:
• Regression analysis that will identify correlations between data (e.g. the device location/geography correlates to battery life).
• Data visualization that can be useful in spotting trends in the data.
• Predictive analytics, which can be particularly useful with large data sets, to identify future trends based on historical data.
• Data mining, which is also normally used with large datasets, to organize data and identify data groups for further analysis.
Benefit-risk indicators and thresholds
The MDR requires that medical device manufacturers not only demonstrate the clinical benefit of their device but also quantify the benefit-risk ratio. The benefit of a device must be shown to clearly outweigh the risk for it to gain market approval. Article 2 (24) of the MDR defines the benefit-risk determination as “the analysis of all assessments of benefit and risk of possible relevance for the use of the device for the intended purpose when used in accordance with the intended purpose given by the manufacturer.”
A PMS system should clearly define benefit-risk calculations and the data used to support them. Post-market surveillance activities are critical in order to re-evaluate and maintain the benefit-risk calculations and determinations of a device throughout its life. Information that is gained through a PMS system can lead to:
• Identification of new risk factors.
• Adjustments to risk frequency and/or severity values based on actual use data.
• Adjustments to established risk calculations based on new “state of the art” technologies becoming available.
• Adjustments to established benefit calculations based on actual use data.
While complaint handling and other feedback tracking are more often described as part of post-market vigilance systems, they play a role in the more proactive post-market surveillance processes as well. A PMS system should define ...
To continue reading this ebook, download the full version.

GUDID: An overview of the FDA's Global Unique Device Identification Database
GUDID is an important source of information as well as a key regulatory requirement for medtech manufacturers who market medical devices, in vitro diagnostics, or medical software in the United States. This article provides an overview of the system, and links to relevant FDA resources you can visit to learn more.
What is GUDID?
GUDID is an acronym for the Global Unique Device Identification Database, a central repository of detailed medical device information created by the FDA. It is often pronounced “Good ID”. The GUDID was implemented as a component of the FDA’s Unique Device Identifier (UDI) requirements, and serves as a digital hub of all the UDI information for all the medical devices that are marketed in the United States.
The GUDID database is designed to help identify and trace all medical devices sold in the U.S., and provides detailed specifications about each device including manufacturer and production information, intended use, safety, and storage and handling requirements. The database is accessible to regulators, manufacturers, healthcare providers, insurers, and the public at large.
GUDID history
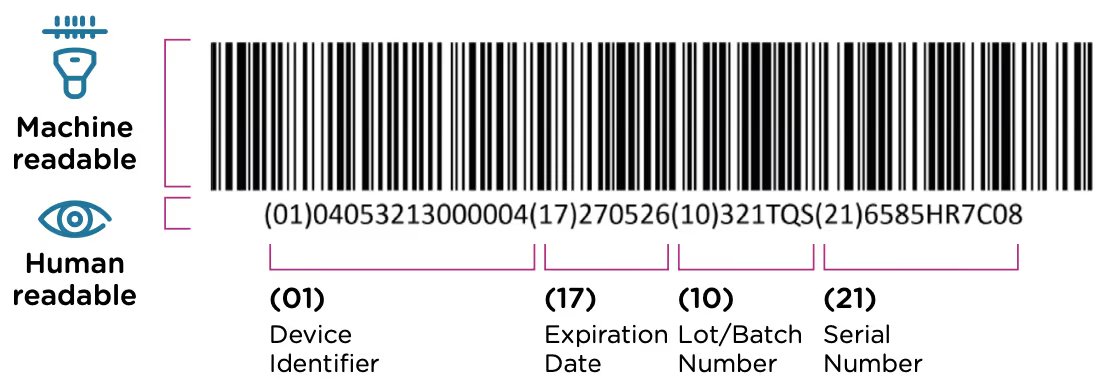
The GUDID was implemented as a part of the FDA’s UDI system. This system requires that each medical device have a unique identification code that is included in the device label (printed on the device itself or its packaging) in both machine and human readable format. An example of a UDI code is included below. The UDI code contains information about the device, the manufacturer, and when/where the device was manufactured.
The FDA’s UDI program was established in 2013, when a rule was issued requiring all medical devices to carry a UDI by 2020. The GUDID database was included with the same regulation, and manufacturers were required to submit all of their UDI information electronically to this database as the requirements came online for different device classes. The overall UDI requirements rollout had the following timeline:
The GUDID database was launched ahead of the first device deadline in December, 2013, and the public access portal AccessGUDID went live in May, 2015.
Who should submit data to the GUDID?
The FDA specifies that the GUDID submission is the ultimate responsibility of the “device labeler”. This is the entity/company who is identified on the device’s label (which also contains the UDI code). So the same entity that attaches the UDI to the device, is also responsible for the electronic GUDID submission. In almost all cases this is the manufacturer of the device, however, it can be the U.S. distributor for the product if they are named on the product’s label.
What data must be submitted to the GUDID?
The information submitted to the GUDID includes all of the device information that is in the UDI code along with additional information about product distribution, product and packaging size, sterilization, and storage and handling instructions. The following information is required to be included with each submission:
- Device identifier information - This includes the device identifier (the first part of the UDI code), a detailed device description, and information about the labeler including the DUNS code, and company name and address.
- Commercial distribution - This includes the distribution status—whether or not the device is in commercial distribution, and the distribution end date—when the device will no longer be distributed.
- Alternative identifiers - If the device has another DI, either a direct marketing DI, a distinct packaging DI, one from another issuing agency, or one that was used previously, this information must be provided.
- Customer contact information - A phone and email address for patients or consumers who have questions about the device.
- FDA codes and listing number - If the device completed a pre-market authorization (PMA) that should be included as well.
- Manufacturing information - Manufacturing date, lot or batch number, serial number, and expiration date for the device.
- Latex information - Whether or not the device or its packaging contains rubber components.
- Device dimensions - What is the clinically relevant size and unit of measure for the device.
- Storage and handling - Requirements and parameters for storage including temperature, humidity, and pressure.
- Sterilization - Whether the device is packaged as sterile or requires sterilization prior to use.
The FDA provides a detailed spreadsheet of data requirements that you can use to prepare your submission.
Creating a GUDID submission
In addition to gathering the required information (and obtaining a UDI code for your device) there are several additional steps to complete in order to create a GUDID submission for your product. First, if you don’t have one, you’ll need to create a GUDID account. The FDA allows you to request an account online. Note that you will need to have a DUNS number for your business. If you don’t have one you can request one from Dun & Bradstreet at no cost.
There are two ways that you can enter your submission. You can do this online through the GUDID Web application. The FDA also allows you to submit your GUDID information all at once using an XML file that complies with Health Level 7 (HL7) Structured Product Labeling (SPL) formats. These submissions are made via the FDA Electronic Submissions Gateway, and require you to set up a gateway account.
In addition, some software providers (like Rimsys) include the ability to make electronic GUDID submission directly from their tools. They provide a system to organize and manage UDI data for the US and other countries, and can ensure that GUDID information for your products is kept up to date.
The global proliferation of UDI regulations
The GUDID was one of the first public databases of medical device information, but many additional countries and regions have followed suit. The European Union, China, South Korea, and Taiwan have all introduced UDI databases and requirements that manufacturers submit records for all of their products sold in-market, and ensure that they are kept up to date.
For more information about global UDI programs and timelines, see our UDI quick reference guide. And you can find more detailed information about the specific requirements in the EU and China in our Ultimate guide to the MDR/IVDR UDI and Ultimate Guide to the China NMPA UDI requirements ebooks.

Rimsys raises $16M Series A to bring regulatory order to the medtech industry
We’re excited to announce that we’ve closed $16M in Series A financing led by Bessemer Venture Partners, with participation from Allos Ventures, Private Opportunities, and Innovation Works. Rimsys was created because there wasn’t a viable regulatory information management (RIM) solution on the market for medtech companies, leaving regulatory affairs (RA) teams to manage increasingly complex work with spreadsheets. The growth that we’ve seen (3X this year), and the work we’ve done with some of the world’s largest medtech companies including Johnson & Johnson, Terumo, Siemens, and the Cooper Companies, makes us incredibly excited about what’s to come.
Regulatory digitization and automation for the medtech industry
The regulatory landscape for medical device, in vitro diagnostic, and medical software products is growing increasingly complex. The implementation of the new European Union Medical Device Regulations in May, to be followed by the In Vitro Diagnostic Regulations next year, brought new general safety and performance, unique device identification, and post-market surveillance requirements that manufacturers must comply with. Research from MedTech Europe predicts that as many as 76% of products will be withdrawn from the market as a result.
Growing complexity isn’t limited to the EU region. This year, Australia has released new essential principles requirements, Canada has expanded post-market requirements, and China has launched a new UDI system. The simple fact is that the largely manual way that RA teams have managed processes won’t work moving forward.
The Rimsys RIM Platform provides an automated, digital alternative to these traditional approaches. It’s a 100% cloud-based software solution that’s specifically designed around medtech regulatory activities and processes.
Rimsys provides a centralized "single source of truth" for all regulatory information and documents. It automates regulatory submissions, including product and UDI registrations, and monitors expiration dates, applicable standards, and regulations for changes that might impact products. It’s a single, integrated solution that supports the full breadth of regulatory activities, and organizes all of it at the individual product level, giving medtech companies unprecedented visibility into and control over their regulatory processes.
New leadership to drive continued growth
We’re also excited to announce new company leadership that will help us through our next phase of growth. We’ve added two new executive leaders with extensive industry experience: Adam Price, former head of post-market surveillance at Philips, and Christine Robertson, former IT leader supporting regulatory at Thermo Fisher Scientific. Adam will lead post-market strategy for Rimsys, developing new offerings to streamline and simplify that part of the regulatory lifecycle. Christine will lead implementation and professional services, bringing best-practices from successful large-scale RIM deployments to all of our customers.
We’ve also added two new board members: Andrew Hedin, Partner at Bessemer Ventures, and Eric Boduch, Co-founder of Pendo, a $2.6B SaaS company that helps companies develop better software products. Both bring a wealth of start-up, SaaS, and industry experience that will be incredibly valuable as we scale the company.
What’s next
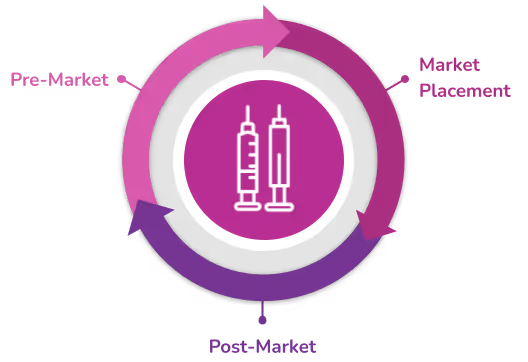
Our goal is to build a comprehensive software platform for medtech regulatory affairs that supports activities across the regulatory lifecycle from pre-market to market placement to post-market surveillance. This year we became the first vendor to offer UDI management directly integrated with product registration data. And we announced a new partnership with Clarivate to bring world-class regulatory intelligence into the Rimsys platform where customers can leverage it directly within automated processes.
We will continue to expand our capabilities at an even faster pace, with new collaborative submission authoring, electronic transmission, regulatory intelligence, document management, and post-market surveillance features coming to the platform. We will also continue to expand our team with a new UK office to better serve the European market, and a number of new roles across the company. If you’re interested in helping medtech companies get lifesaving products to market more quickly, we’d love for you to join our team.
Learn more about Rimsys
We’d love to show you how the Rimsys RIM Platform can help medtech companies streamline processes across the regulatory lifecycle, strengthen global compliance, and get new products to market faster. Contact us to schedule a free custom demo.

RIM 101: what is regulatory information management?
Regulatory Information Management (RIM) refers to a category of software solutions that are designed to support and streamline the activities of regulatory affairs (RA) teams. For most teams they are a net-new category of software, and generally replace manual processes that are paper-based or run using traditional productivity software (spreadsheets and docs). RIM systems first emerged to support pharmaceutical regulatory activities, but in recent years medtech-focused solutions have hit the market as well.
Given their general new-ness, especially for medtech RA teams, it’s not surprising that many teams are unfamiliar with the technology. In our, admittedly informal, survey of RAPS 2021 attendees, only 11% of respondents said they currently use a RIM system, and 33% had no knowledge of the category at all. This article provides some background on what RIM systems are, and what they do to help medtech RA teams operate more effectively.

The role of regulatory affairs in medtech
To understand RIM systems, first we have to look at the role of regulatory affairs. In medtech, which includes medical devices, in vitro diagnostics, and medical software, RA teams play a critical role across a product’s lifecycle.
Before products are released for sale, RA teams work closely with research and development (R&D) teams to ensure that a new product meets necessary local requirements to be legally marketed in the desired target markets. There are over 113 different regulatory regimes around the world that medical devices are subject to. While there are many similarities, RA teams must understand the nuances between countries and guide R&D to ensure that products are developed accordingly.
Once products obtain market clearance, RA teams switch to monitoring mode to ensure that products can remain on the market. This includes keeping track of expiration dates and certificates, any changes in regulations or international standards that could impact the product, and any changes in the product or it’s technical documentation. Health authorities in many countries regularly perform product audits, so keeping all information in order and up-to-date is an important part of regulatory work.
RA teams usually take the lead on post-market surveillance activities as well, working closely with their quality assurance (QA) counterparts. They track adverse events and complaints, compiling this information from public and internal sources, and ensure that the data is reported appropriately to health authorities. Not all markets require extensive post-market surveillance for medical devices, but these regulations are becoming more common. Both the EU and Canada have recently implemented expanded surveillance requirements including the need for regular summary reporting to continuously confirm product performance and safety.
The information challenge
All of the regulatory activities highlighted in the previous section are repeated for every individual product the company sells in every regulated country or region. And, all of these activities are highly dependent on specific information. To do their jobs effectively, medtech regulatory affairs professionals need insight into global regulations and standards, detailed product specifications, testing, performance, and safety data, and a full record of all regulatory registrations and processes.
The problem is that this information is often scattered across the company. It’s stored in multiple systems, (sometimes physical) documents, and individual employees’ heads. Because this information is so scattered, RA professionals can spend up to 50% of their time just looking for things, and simple requests such as identifying whether a product has clearance to be marketed in a specific country can take days to complete.
How RIM systems can help
At a fundamental level, RIM systems are about helping RA teams corral and manage all of the information they need to do their jobs. RIM systems serve as a “single source of truth” for RA teams. They store and manage regulatory documents, integrate with systems across the company, and create a traceable record of all regulatory activities. All of this information is linked to individual products and countries or regions, making it much easier to find.
All of the collected information in a RIM system can be used to streamline regulatory activities across the product lifecycle. Before products are released, they provide access to regulatory intelligence, including market entrance requirements, that RA teams can use to guide product development and regulatory submissions. RIM systems also provide a collaborative digital hub where teams can author and assemble supporting documentation for new regulatory submissions.
For products currently on the market RIM systems can monitor registration expiration dates, and track changes in relevant standards and regulations to identify potential product impacts. This automated monitoring can give RA teams an “early warning”, and allow them to accommodate changes that might impact the selling status of a product.
RIM systems can also help with post-market surveillance activities. They can collect and centralize post-market data analytics, and facilitate planning and active surveillance activities to meet the most current regulatory requirements. These systems can also ensure that actions and conclusions drawn from the post-market surveillance process are consistently applied throughout the quality management system. And, the same authoring capabilities used to assemble pre-market submissions can be used for post-market reporting and communication with regional regulatory authorities.
Project planning, tracking, and management
Underpinning all of these capabilities is a full set of project features that allow RA teams to effectively manage and track their activities. This can include project request features that allow internal teams or 3rd-party partners such as local distributors to request specific regulatory activities or information. RIM systems also provide project task management, approval workflows, and digital signature capabilities that are fully auditable, and 21 CFR Part 11 compliant.
RIM systems also provide detailed reporting in the form of customized dashboards and registration, product, standards, and documentation reports. These reports offer at a glance monitoring of key information and detailed visibility into regulatory status and activities. For many teams this level of visibility is new, and allows them to fully measure, benchmark and report on their activities to company leadership.
The impact of RIM systems
RIM systems can have a tremendous impact on RA teams. By centralizing information they improve team productivity by ensuring that up-to-date information is always easily available and consistently applied. By automating workflows like new submission creation, or essential principles/GSPR table assembly they ensure that work gets done quickly and in-line with country/region requirements. RIM systems also provide more visibility into regulatory activities, allowing teams to benchmark and more accurately forecast the time required for new market clearance, and other product milestones.
To the company, the increased regulatory efficiency and effectiveness means reduced revenue risk from noncompliance or having to pull products from market, stronger, more confident global regulatory compliance, and ability to get new products to market much more quickly.
To learn more about RIM systems, their key capabilities, and if your organization could benefit from bringing one onboard, read our RIM System Buyer’s Guide for Medtech Companies.

Regulatory information management (RIM) systems and organizational change management
At first glance, the juxtaposition of RIM and change management seems a little strange. One is a software tool and the other a management discipline, but one of the things we’ve seen across RIM deployments is that it’s difficult to have one without the other. For many regulatory affairs teams, a RIM system isn’t simply a tool, it’s a digital transformation. This means that there’s a broader set of organizational considerations and actions that need to surround the implementation of a RIM system to ensure its success. Remember that 70% of digital transformation initiatives fail.
RIM systems are a disruptive technology
Disruptive? Really? Aren’t RIM systems supposed to streamline regulatory activities, and improve team productivity? Yes they definitely provide these benefits, but they also require a change in how the team works. Most RIM implementations aren’t replacing existing software, they’re replacing manual processes. In our experience, Rimsys is displacing registrations that are managed via spreadsheets, and sometimes even paper-based processes.
This means that the way that teams have managed processes is changing significantly. While it’s likely that teams are struggling to operate effectively (there’s usually some organizational pain that leads to a RIM evaluation), there’s also discomfort with the change. RA team members are proficient in their work, they know how to get things done, and likely have systems they’ve created to cope with the inefficiencies in their current processes.
Regardless of department or industry, automation initiatives can lead to employees feeling threatened with obsolescence, lacking direction, and afraid of being replaced. In medtech regulatory affairs this is rarely the case. Most companies have to invest heavily in external consultants just to keep pace with the current workload. In fact, large medtech companies regularly outsource 50% or more of their regulatory activities. This doesn’t mean that team members won’t experience these insecurities. That’s why it’s important to have a change management strategy in place to support any RIM rollout.
A RIM change management strategy
All of these factors mean that RIM implementation that doesn’t have an accompanying change management strategy won’t see the same level of success, or deliver on expected outcomes. The good news is that there are a universal set of tactics to support effective change management that can be easily applied in this scenario. Here are 4 steps that you can take to lay the groundwork for a successful RIM implementation.
Step 1: start at the top
Teams that are in the process of acquiring a RIM system likely already have leadership support, but it’s important that your senior leaders have a visible presence in the process. This means issuing communications, participating in kick-off meetings, and being available to answer questions. This applies both to RA leaders and those in adjacent departments like QA and IT as well.
The visible support reinforces the idea that leadership teams are aligned and fully supportive of the changes taking place. It affirms that RIM is a strategic priority for the company, and helps to alleviate any fear or anxiety about the change. Leadership support also helps to signal to teams that they’ll be supported as they go through the implementation process, and that work will be prioritized.
Step 2: communicate early and often
RA teams are busy—often very busy. This is typically why a RIM system is being implemented in the first place. However, when teams are really busy, it’s really easy for communications to fall through the cracks. This means that plans and timelines for a RIM implementation need to be communicated more than once.
Communications should emanate from leadership teams (see step 1), and be candid about coming changes, the reasons for them, and the expectations from team members as the project moves forward. Leaders should encourage communication that moves in both directions, and be open to feedback from team members. Companies should look to create channels for RA team members to reach out with any comments or concerns.
Step 3: strive to minimize disruption
While there’s no way to completely eliminate the disruption associated with a new RIM system—it will fundamentally change the way a RA team works there’s no way around it—there are ways to minimize disruption. There first part of this is making sure you’re communicating enough about the project (see step 2). Team members are much more receptive to change if they aren’t blindsided by it.
It’s also helpful to take steps to make sure that team members have an opportunity to learn about the RIM systems throughout the acquisition and implementation process. Bring team members into product demonstrations, and let them ask questions about solutions that are being evaluated. Don’t wait to run training sessions until the RIM system is fully implemented. These can run in parallel. With this approach the whole team feels invested in the solution, and is fully ramped to start running at the end of implementation.
Step 4: lay the groundwork for continuous improvement
This article discusses change management from the perspective of a discrete event—the acquisition and implementation of a RIM system. However, RA teams shouldn’t look at change as something with fixed start and end, but rather as something continuous. RIM systems today represent one way that RA teams can embrace digitization and automation to improve how they work. There will be many additional opportunities as regulations, regulatory bodies, and technology evolve.
In recent years we’ve seen an expansion of UDI requirements for medical devices across markets. We’ve seen more stringent requirements for post-market surveillance. And we’ve seen the growing adoption of digital pathways for regulatory submissions and other interactions with health authorities. For many teams, a successful RIM implementation is just the first step on what will be a broader organizational transformation.
Successful changes for RIM and beyond
RIM systems can provide enormous benefits to RA teams, but only if they’re fully implemented and adopted. While deep in the weeds of requirements gathering and vendor evaluations it’s easy to overlook the fact that moving from traditionally manual processes to automated ones in a RIM system represents a significant organizational change. As a part of any RIM acquisition initiative, teams should fully understand their change management needs, and take steps to address them in concert with software selection.
Having teams fully onboard and supportive of the initiative makes them much more likely to adopt the final solution. Engaging in this way also allows you to plan for, and prioritize the resources needed for the implementation phase—leading to faster time to value for the project. Ultimately organizational change will and should be something that RA teams are comfortable with. The practices adopted with a RIM implementation can be used to support future digitization and automation across all RA activities.
To learn more best practices around RIM sourcing and implementation including an organizational self-assessment, detailed overview of capabilities, and a worksheet you can use for vendor evaluations, check out our RIM Buyer’s Guide for MedTech Companies.
A primer on medical device classification
While it may seem simple, medical device classification can be a challenging task for many medical device and IVD manufacturers. Device classes for specific regions and countries have a number of small variations, and each of those variations can impact the process by which a device obtains market clearance. Getting it wrong can lead to delays in getting to market. This article explores the classification systems for three major markets, and their associated regulations.
An important component of achieving regulatory approval is the appropriate classification of a medical device or in vitro diagnostic device, according to the specific regulations within a country or region. Product classifications are related to the intended use of the product and the perceived risk that it poses to a patient using the device. While this general approach is pretty standard across all regions, there are many small variations in different country classification systems that can impact how a device is regulated. It would be much easier if there was one global classification system that everyone followed.
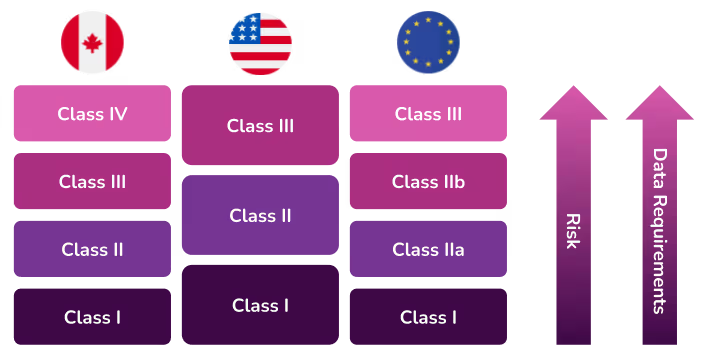
However, since there are different guidelines to classifying a medical device (per country), we’ll dig into the most popular classification systems—Canada, the European Union and the United States. These three are globally perceived to have strong, thorough, and trusted quality and regulatory systems. Their approaches are often mirrored or used as proxies for market clearance in other countries.
Canada
The Canadian Medical Devices Regulations include guidelines that classify devices into four risk classes. If a medical device can be classified into more than one class, the class representing the higher risk always applies.
- Class I devices do not require a medical device licence to be sold in Canada, but manufacturers, distributors and importers of these devices are required to obtain an establishment licence.
- Class II requires a medical device licence
- Class III requires a medical device licence
- Class IV requires a medical device licence
Some examples of different classes of devices in Canada include:
European Union
One of the main changes introduced with the new MDR/IVDR regulations are new classification rules for medical devices and in vitro diagnostic devices. If you have gone through the process of getting your medical device in the European market before, you might find it more difficult with the new EU MDR rules. For example, a new medical device you want to bring to market might now fall into a higher classification than it would have previously (under the MDD), and therefore require more testing, updates to documents, quality approvals, etc.
The new EU MDR brings the classification of medical devices in Europe more in line with international regulations, specifically the United States. These updated rules are listed in MDR 2017/745 for devices and IVDR 2017/746 for in vitro diagnostic products. As with Canada, if a medical device can be classified into more than one class, the class representing the higher risk always applies.
The EU has recently released a new guidance document MCDG 2021-24 to assist device manufacturers with device classification questions.
Class I – this classification is for the lowest risk device. Most medical devices in this category do not require a conformity assessment from a Notified Body so instead, they can be self-assessed. However, manufacturers must still complete a Technical File as part of the approval process.According to MDCG 2019-15, there are three subclasses under Class I. Unlike most Class I devices, these will require the involvement of a Notified Body.
- Class Im: a product with a measuring function
- Class Is: a product that is sterile
- Class Ir: a product that is a reusable, surgical instrument
Class IIa – this classification is for a medium risk device. A conformity assessment by a Notified Body is required for this classification.
Class IIb – this classification is for medium-to-high risk devices. A conformity assessment by a Notified Body is required for this classification.
Class III – this classification is for the highest risk devices. A conformity assessment by a Notified Body is required for this classification.
Examples of different classes of devices in the European Union include:
In Vitro Diagnostic Devices:
Class A – this classification is for the lowest risk in vitro diagnostic devices. Most IVD devices in this category do not require a conformity assessment. Instead, they can be self-assessed.
Class B – this classification is for medium risk in vitro diagnostic devices. A conformity assessment by a Notified Body is required for this classification.
Class C – this classification is for medium-to-high risk in vitro diagnostic devices. A conformity assessment by a Notified Body is required for this classification.
Class D – this classification is for the highest risk in vitro diagnostic devices. A conformity assessment by a Notified Body is required for this classification.
Examples of the different in vitro diagnostic device classes in the European Union include:
United States
In the United States, the Food and Drug Administration (FDA) is responsible for overseeing the safety of medical devices. The FDA has established classifications for approximately 1,700 different types of devices and grouped them into 16 medical specialties referred to as panels. All three classes of devices are subject to General Controls which are the baseline requirements of the Food, Drug and Cosmetic (FD&C) Act.
- Class I – General Controls (with or without exemptions)
- Class II – General Controls and Special Controls (with or without exemptions)
- Class III – General Controls, Special Controls and Premarket Approval
You are permitted to classify your own medical device based upon the FDA guidance documents and set regulations. However, if you wish for the FDA to assist with establishing your classification you can submit a 513(g) Request for Information. Note that there is a user fee associated with a 513(g) Request.
The device class determines which type of premarketing submission/application is required for market clearance.
In some instances, you do have the opportunity to reclassify your product after it’s been released to the market. The regulatory class of a device type, as defined by the Federal Food, Drug and Cosmetic Act (FD&C Act), may be changed through petition to the FDA. This process is only applied to a device type though, not to an individual device.
Examples of medical device classification in the US include:
Getting classification correct
Medical device classification is simple in that each country and region generally follows the same classification approach, and complex in that minor differences can change how a device is classified across markets. Understanding how a device is classified is one of the critical first steps regulatory affairs teams need to take when entering a new market, as medical device class often determines the pathway to market.
For example, in the EU classification can mean the difference between self-certification and a required conformity assessment from a Notified Body. In the US, classification can mean the difference between a 510(k) or PMA process for market clearance. Getting classification correct can ensure a smoother and faster route to market.
To learn more about market clearance processes for medical devices in the US, check out the Beginner’s Guide to the 510(k).

MDSAP - the ultimate guide to the medical device single audit program
This article is an excerpt from The ultimate guide to the medical device single audit program (MDSAP) ebook.
Table of contents
- What is MDSAP?
- History of MDSAP
- Who is responsible for the MDSAP?
- How does an MDSAP audit work?
- Audit sequence
- You got a nonconformity – now what?
- What does an MDSAP audit cost?
- Why choose the MDSAP certification process?
- Potential disadvantages of the MDSAP
- Ready to participate? – Here’s how to get started
- Completing a successful MDSAP audit
The Medical Device Single Audit Program (MDSAP) was designed and developed to allow a single audit of a medical device manufacturer to be applied to all country markets whose regulatory authorities are members of the program. The MDSAP provides efficient and thorough coverage of the standard requirements for medical device manufacturer quality management systems, and requirements for regulatory purposes (ISO 13485:2016). In addition, there are specific requirements of each medical device regulatory authority participating in the MDSAP that must be met:
- Conformity Assessment Procedures of the Australian Therapeutic Goods (Medical Devices) Regulations (TG(MD)R Sch3)
- Brazilian Good Manufacturing Practices (RDC ANVISA 16)
- Medical Device Regulations of Health Canada (ISO 13485:2003)
- Japan Ordinance on Standards for Manufacturing Control and Quality Control of Medical Devices and In Vitro Diagnostic Reagents (MHLW Ministerial Ordinance No 169)
- Quality System Regulation (21 CFR Part 820), and specific requirements of medical device regulatory authorities participating in the MDSAP program.
This means that a report from a single MDSAP audit of a medical device manufacturer would be accepted as a substitute for routine inspections by all the member Regulatory Authorities (RAs) across the world. There are currently five participating Regulatory Authorities (RA) representing the following countries: Australia, Brazil, Canada, Japan and the USA.

In April, 2021, the RAs released an “Audit Approach” document (MDSAP AU P0002.006) that combines the formerly separate MDSAP Audit Model and Process Companion documents into a single guidance document. It includes guidance for assessing the conformity of each process and includes an audit sequence, instructions for auditing each specific process, and identifies links that highlight the interactions between the processes.
In March 2012 the US FDA announced that they had approved a final pilot guidance document “Guidance for Industry, Third Parties and Food and Drug Administration Staff: Medical Device ISO 13485:2003 Voluntary Audit Report Submission Pilot Program.” This allowed the owner or operator of a medical device manufacturing facility to be removed from FDA’s routine inspection work plan for 1 year upon completing a ISO 13485:2003 audit. This guidance document went into effect in June 2012, and was intended as an interim measure while a single audit program was being developed.
This pilot program was not very successful and few companies signed up because they did not see any advantage in participating. The manufacturer had to pay for a third party to inspect their facilities, generate a report, and share the inspection results back to the FDA. Many companies were reluctant to contract “someone else” to perform their inspection when they could easily wait for the FDA to conduct an inspection for free.
During its inaugural meeting in Singapore in 2012, the International Medical Device Regulators Forum (IMDRF) appointed a working group to develop a set of documents for a harmonized third-party auditor system. Hence, the “Medical Device Single Audit Program” (MDSAP) was formed. The concept was similar to the FDA’s original idea of creating a third-party auditor to help reduce their workload of performing regulatory audits of medical device manufacturers’ quality management systems. This new approach would consist of a single audit that would review regulatory QMS compliance, conducted by a third-party, who would later be called an Auditing Organization (AO).
From January 2014 to December 2016, five countries participated in a Medical Device Single Audit Program Pilot. In June 2017, a report was generated summarizing the outcomes of prospective “proof- of-concept” criteria established to confirm the success of the program. The outcomes are documented in the final MDSAP Pilot Report and recommended that the program become fully active and open to any manufacturer who requested this type of audit.
The governing body of the MDSAP is the Regulatory Authority Council (RAC), which is composed of two senior managers (and a few other staff members) from each participating RA. They are responsible for executive planning, strategic priorities, setting policy, and making decisions on behalf of the MDSAP International Consortium. The RAC also reviews and approves documents, procedures, work instructions, and more. The mission of the MDSAP International Consortium is to jointly leverage regulatory resources to manage an efficient, effective, and sustainable single audit program focused on the oversight of medical device manufacturers on a global scale.
Other international partners that are involved in the MDSAP include:
MDSAP Observers:
- European Union (EU)
- United Kingdom’s Medicines and Healthcare products Regulatory Agency (MHRA)
- The World Health Organization (WHO) Prequalification of In Vitro Diagnostics (IVDs) Program
MDSAP Affiliate Members:
- Argentina’s National Administration of Drugs, Foods and Medical Devices (ANMAT)
- Republic of Korea’s Ministry of Food and Drug Safety
- Singapore’s Health Sciences Authority (HSA)
The observers and affiliate members are not the same as the participating member RA’s. The observers simply observe and/or contribute to RAC activities. Affiliate members, on the other hand, are interested in engaging in the MDSAP program and are subject to certain rules. They are only given access to a certain level of information about the manufacturers, audit dates, and information in audit reports.
They are also invited to attend sessions that are open to members, observers, and affiliates only.
Audits can also be conducted by MDSAP participating RAs at any time and for various reasons including:
- "For Cause" due to information obtained by the regulatory authority
- as a follow up to findings from a previous audit
- to confirm the effective implementation of the MDSAP requirements
The purpose of audits conducted by the RAs is to ensure appropriate oversight of the AOs MDSAP auditing activities. The AOs are appointed by the RAs and a list of the currently approved AO’s is published on the FDA website. Most AOs offer a broad range of management system certification services, beyond just medical devices. Manufacturers should verify that prospective AOs are clearly trained and perform MDSAP audits of medical devices.
AOs have the final word as to whether a manufacturer has met the requirements for the MDSAP during the execution of the audit and generation of the associated reports summarizing the results. MSDAP RAC participating RAs have the final decision regarding all development, implementation, maintenance, and expansion activities associated with the program.
Although an unannounced visit by an AO is rare, it can happen in circumstances where high-grade nonconformities have been detected.
To continue reading this eBook including a detailed look at the MDSAP audit process and grading, pros and cons of the approach, and how to get started please register to download the full version.
