


Featured
Rimsys Announces Rimsys AI to Eliminate Repetitive Tasks and Enhance Decision-Making for MedTech Regulatory Teams
Rimsys, the leading Regulatory Information Management (RIM) platform for the MedTech industry, today announced the launch of Rimsys AI, a suite of embedded artificial intelligence (AI) agents.
.avif)
2023 Regulatory performance report
Today at Rimsys, we unveiled the 2023 MedTech Regulatory Performance Report, a new set of insights into the state of medtech regulatory affairs. Compiled based on interviews with 200 regulatory professionals and executives, the study provides a detailed look into how regulatory teams are staffed, their processes, the tools they use, and ultimately how they perform.
Why did we create this study? There were two driving factors behind the research. The first was a common theme that we heard from a number of our customers: Regulatory leaders don’t have clear data and benchmarks. They don’t necessarily know how long a new market submission should take, and how to plan for or assess the work of their teams. While other studies look at the medtech industry broadly or the state of the regulatory profession, this study tries to build a comprehensive resource for regulatory (and company) leaders.
The second factor was really for ourselves and the team at Rimsys. As a company building solutions specifically for medtech regulatory affairs, we wanted more insight into where companies were successful, where they struggled, and where we can add value.
What did we find? Regulatory teams perform a lot of hero work and rate themselves highly for their accomplishments. At the same time there is a lot of opportunity for process improvements, and companies that invest in digital transformation for regulatory affairs see better performance.
Regulatory professionals are superheroes
Regulatory teams are generally pretty small. Most companies have less than 10 full-time regulatory professionals. These small teams complete an enormous amount of work. Last year on average, RA teams completed 50 license renewals, 50 license updates, and 10 new market submissions. This is impressive output.
Digging a bit under the covers, we found that this output relied heavily on the support of external consultants. 90% of companies use consultants to keep pace with their regulatory workload. Front-line employees also struggle with burnout. They were much more likely to report feeling under-resourced than regulatory leaders.
But process problems persist
A lot of regulatory work remains extremely manual. 70% of regulatory teams spend half their time or more on repetitive administrative tasks. All of this manual work increases the frequency of errors and required rework. 61% of companies reported a major non-compliance incident in the past 2 years.
Manual work also makes it difficult to complete regulatory projects in a timely fashion. Teams completed a lot of projects, but each took a long time. Over half of all companies spend 4 months or more on license renewals, license updates, and new market submissions.
Moving regulatory affairs forward
As regulatory requirements become more complex, there’s a natural question about how teams will work moving forward. MDR & IVDR in Europe have significantly increased the regulatory workload required to bring and keep products on the market. Will organizations be able to keep pace with the same resources, tools, and processes?
No, and the performance report shows that medtech companies are investing to improve their regulatory capabilities. The majority of companies are planning to increase the sizes of their RA teams in 2023, and 40% expect to increase their investments in regulatory software. Companies are increasingly adopting specialized software to better support regulatory processes.
Dig into the survey results
The full survey results provide insights into more aspects of regulatory performance. They show that companies need to take a deeper look into their processes and how regulatory resources are allocated. There are two ways to learn more:
- Visit the survey page to see the full results (the survey whitepaper can be downloaded at no cost)
- Watch the recording of our webinar with PA Consulting. We discuss the survey results in more detail and share our regulatory predictions for 2023


Post-market surveillance for medical devices in the European Union
This article is an excerpt from Post-market surveillance for medical device in the European Union.
Table of Contents
- What is post-market surveillance?
- What classes of medical devices require post-market surveillance?
- Components of a successful post-market surveillance plan
- PMS data requirements
- Post-market surveillance system goals
- Required post-market surveillance reporting
- Embracing post-market surveillance as an integral part of your quality program
- Getting started with post-market surveillance
Post-market surveillance (PMS) is designed to monitor the performance of a marketed medical device by collecting and analyzing field use data. Article 10 of the EU MDR and IVDR requires all device manufacturers to have a post-market surveillance system in place. The main elements of the PMS are laid out in Article 83, and additional details for lower-risk and higher-risk devices are covered in articles 84 and85, respectively.
In general, a PMS system consists of both proactive activities and reactive, or vigilance, activities. While post-market surveillance and vigilance are sometimes used interchangeably, vigilance consists of separate activities that feed post-market surveillance programs.
Post-market surveillance systems are used to collect and analyze data not only about the manufacturer’s device but also about related competitors’ devices that are on the market. Data collected through PMS procedures is then used to identify trends that may lead to, among other things, quality improvements, updates to user training and instructions for use, and identification of manufacturing issues.
Note that “market surveillance” encompasses activities performed by a Competent Authority to verify MDR compliance, and should not be confused with the topic of this ebook,“post-market surveillance," which is performed by the manufacturer.
All medical devices marketed in the EU require some level of post-market surveillance, and all medical device manufacturers must implement a post-market surveillance system (PMS). The requirements of the PMS, however, vary and should be “proportionate to the risk class and appropriate for the type of device” (MDR Chapter VII). In particular, the type and frequency of reporting vary based on a device’s risk class.
A post-market surveillance plan (PMS) is an integral part of a manufacturer’s quality management system and provides a system for compiling and analyzing data that is relevant to product quality, performance, and safety throughout the entire lifetime of a device. The PMS should also provide methods for determining the need for and implementing any preventative and corrective actions. A PMS system should include and define:
Surveillance data sources
With the increased focus on proactive risk identification in the MDR, it is important to design post-market surveillance systems that actively acquire knowledge and detect potential risks. It is not sufficient to rely solely on spontaneous reporting by healthcare providers, patients, and other stakeholders.
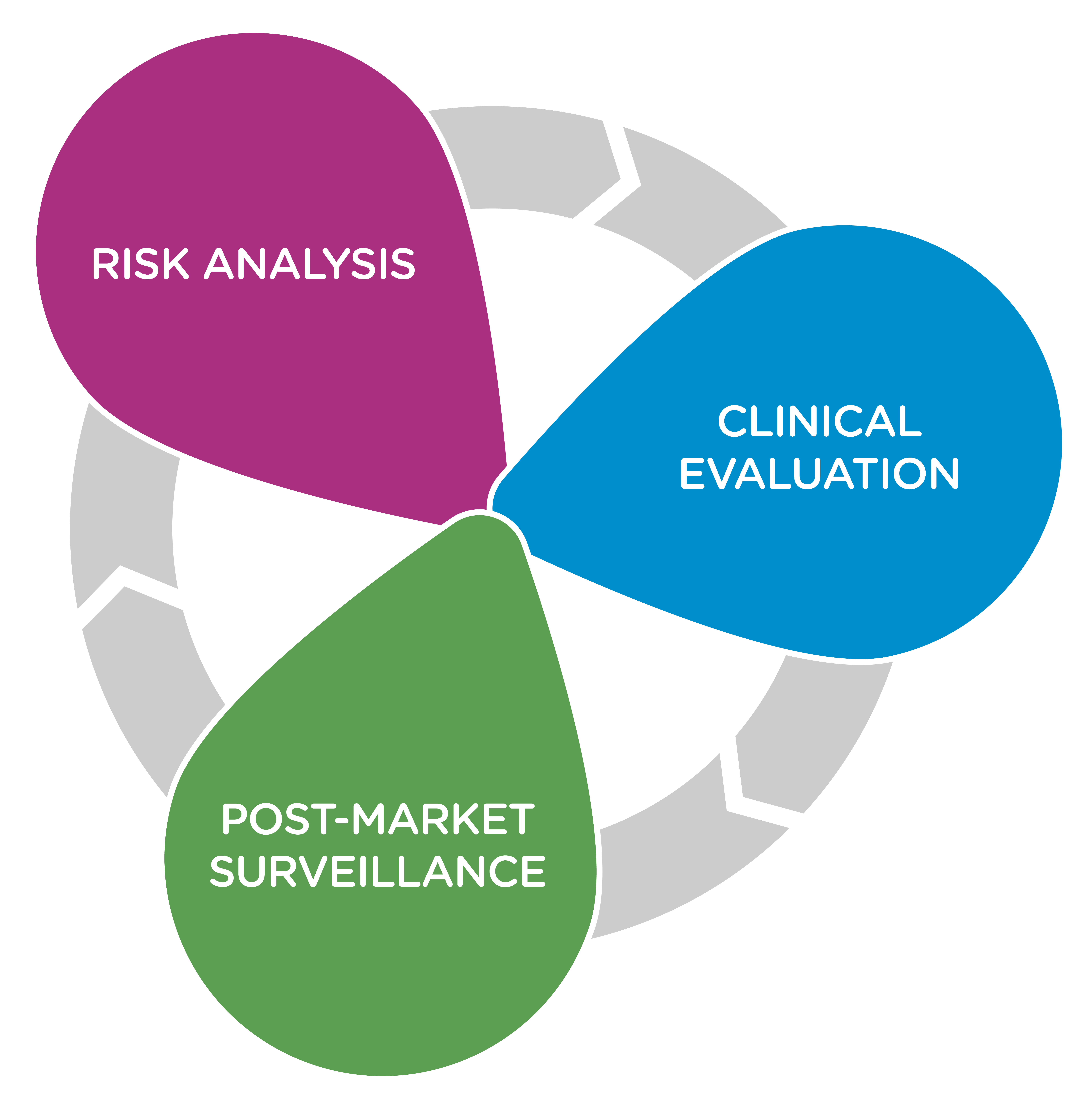
In addition to information coming from Clinical Evaluation Reports and complaint and adverse event reporting, typical sources of surveillance data include:
• Social media networks: Because many of your stakeholders may be communicating on social media networks, it is important to employ social listening techniques and/or tools to identify issues and concerning trends as they develop.
• Industry and academic literature: Any studies, academic papers, and other literature that addresses similar devices or the specific use cases for which your device is designed should be evaluated. In particular, risk factors and adverse events identified with similar devices should be closely examined. It is also important to identify newer technologies that may affect the benefit-risk ratio and establish a new definition of “state of the art” for the device type.
• EUDAMED: While the European Database on Medical Devices (EUDAMED) is not yet fully functional, it is intended to provide a living picture of the lifecycle of all medical devices marketed in the EU. Manufacturers should take special care to consider information for similar devices made available through the EUDAMED system in the future.
• Registries: Patient, disease, and device registries can provide information that informs the clinical evaluation process which provides input into the post-market surveillance system.
Data analysis methodology
A well-defined data analysis methodology will accurately identify trends and lead to defendable decisions in the application of post-market experience. Once the necessary information has been identified and collected, and potentially cleaned of incomplete or otherwise unusable data, the data needs to be analyzed.
The goal is to identify meaningful trends, correlations, variations, and patterns that can lead to improvements in the safety and efficacy of the device. There are many data analysis tools available that can assist with:
• Regression analysis that will identify correlations between data (e.g. the device location/geography correlates to battery life).
• Data visualization that can be useful in spotting trends in the data.
• Predictive analytics, which can be particularly useful with large data sets, to identify future trends based on historical data.
• Data mining, which is also normally used with large datasets, to organize data and identify data groups for further analysis.
Benefit-risk indicators and thresholds
The MDR requires that medical device manufacturers not only demonstrate the clinical benefit of their device but also quantify the benefit-risk ratio. The benefit of a device must be shown to clearly outweigh the risk for it to gain market approval. Article 2 (24) of the MDR defines the benefit-risk determination as “the analysis of all assessments of benefit and risk of possible relevance for the use of the device for the intended purpose when used in accordance with the intended purpose given by the manufacturer.”
A PMS system should clearly define benefit-risk calculations and the data used to support them. Post-market surveillance activities are critical in order to re-evaluate and maintain the benefit-risk calculations and determinations of a device throughout its life. Information that is gained through a PMS system can lead to:
• Identification of new risk factors.
• Adjustments to risk frequency and/or severity values based on actual use data.
• Adjustments to established risk calculations based on new “state of the art” technologies becoming available.
• Adjustments to established benefit calculations based on actual use data.
While complaint handling and other feedback tracking are more often described as part of post-market vigilance systems, they play a role in the more proactive post-market surveillance processes as well. A PMS system should define ...
To continue reading this ebook, download the full version.

A look at the FDA Total Product Life Cycle Advisory Program (TAP)
The Total Product Life Cycle Advisory Program (TAP) is a voluntary pilot program launched by the FDA’s Center for Devices and Radiological Health (CDRH) in October 2023. The TAP Pilot is one of the commitments between the FDA and industry as part of the MDUFA V reauthorization, which aims to provide faster patient access to safe and effective medical devices, increase innovation, improve patient safety through enhanced surveillance and data collection, and provide a more efficient regulatory process for FDA and industry.
Taking a medical device from concept to commercialization in the United States is often a long and challenging process that involves participation and adoption from FDA, clinicians, payers, and patients. The TAP program is addressing the obstacles that device manufacturers often encounter throughout this process with:
- Early and frequent interactions: FDA will provide more opportunities for sponsors to interact with the agency early in the development process, which can help to identify and address potential issues early on.
- Strategic input from stakeholders: The program will involve input from a variety of stakeholders, including clinicians, patient advocates, and payers, which can help to ensure that the development of new devices is meeting the needs of patients and the healthcare system.
- Proactive, strategic advice from CDRH: FDA will provide proactive and strategic advice to sponsors throughout the development process, which can help to reduce the risk of regulatory delays.
Currently, TAP program membership includes the companies or individuals developing the medical devices, the medical device sponsors, dedicated staff within the CDRH, stakeholders consisting of clinicians, patient advocates, payers, and academic experts, and independent advisors. However, It is unclear if independent advisors will continue to be part of the program as TAP expands. Additionally, specific individuals involved in the TAP program at a given time will vary based on the device being developed and the stage of the development process.
While currently still in its pilot phase, the TAP program is open to a limited number of medical devices. To be considered for the program, device manufacturers must have breakthrough designation with no previous pre-submission meetings. The TAP program started with 15 cardiovascular devices last fall and is now at 31 enrolled devices as of February 2024. Enrollment could reach as high as 60 devices by the end of 2024.
As part of the MDUFA V reauthorization, the TAP Program shares the goal of facilitating the development of high-quality, safe, effective, and innovative medical devices. Additionally, the TAP Program strives to reduce device development time and costs through early and frequent feedback from FDA, increase innovation with more predictable and efficient regulatory pathways for new devices, and improve patient access to new devices.
Overall, the TAP program’s focus is on improving the medical device landscape by addressing various challenges and opportunities throughout the product lifecycle. The program's success will be measured by its ability to expedite development, foster innovation, ensure device quality, and ultimately, improve patient access to these potentially life-changing technologies. For more information about the TAP program and enrollment in it, visit FDA’s website.
_thumbnail.avif)
Are FDA risk classifications and submissions any different for SaMDs? [VIDEO]
The number of software as a medical device (SaMD) is growing and with it are questions about how to effectively obtain market clearance for them. One question we hear often is, “Are FDA risk classifications and submissions any different for SaMDs?” Currently, the FDA is regulating SaMDs the same way it’s regulating traditional medical devices. As a result, you’ll still have the same three risk classifications, Class I, Class II, and Class III.
The submission process is also the same. Most Class I devices are 510(k) exempt, and most class II devices would fall under a 510(k) or De Novo submission depending on whether or not substantial equivalence can be made to another US-marketed device. Most Class III devices require PMA submissions.
There have been discussions about FDA pre-certification programs and following IMDRF guidelines for SaMDs, which would alter the submission process and also the risk stratification of SaMDs. However, none of these discussions have matured. The FDA continues to mirror their risk classification and submission guidelines for SaMDs and traditional medical devices.
Watch the full answer to this question from our recent panel discussion with subject matter expert, Prabhu Raghavan of MDQR Solutions, below.
You can also download the full replay here to get answers to other common SaMD questions such as:
- How is the FDA regulating AI/ML in SaMDs?
- What is a Predetermined Change Control Plan (PCCP) for machine learning-enabled medical devices?
- What cybersecurity considerations sh ould be made when taking SaMDs to market?

An introduction to standards for medtech companies
A standard is a published document that is established by consensus and is approved by a recognized body (ISO, IEEE, UL, etc.). It outlines requirements, specifications, guidelines, or characteristics that are used in a repeated way to ensure that materials, products, processes, and services are developed for a specific purpose. Think of it as a formula for an agreed upon way of doing something that establishes the best way of performing a function. It could be developing a product, managing a process, or even supplying materials to a manufacturer.
Why are standards important?
Standards enable technology to work seamlessly across industries and markets and help to build consumer trust that products and services are designed to work together in an efficient way. They form the fundamental building blocks for product development by establishing consistent requirements that can be universally applied, practiced, and understood. For example:
- Quality standards reduce product failures on the assembly line.
- Environmental standards reduce environmental impacts, reduce waste, and provide sustainability.
- Health and safety standards reduce accidents in the workplace.
- Food safety standards prevent food from being contaminated.
To ensure standards stay relevant and are aligned with technology changes, many standards organizations require that their standards be reviewed periodically and updated as necessary.
Is an industry standard the same as a regulation?
No, but there is a very close relationship between the two. Simply put, a standard is a guideline whereas a regulation includes laws. Industry standards are used voluntarily (although strongly encouraged) while regulations are not voluntary because they are a requirement from a government agency or similar authority, i.e. ISO 13485 is a standard and building codes are regulations.
- Standards are technical documents, driven by consensus that are crafted by experts.
- Regulations are sometimes based on standards, created by a variety of individuals and entities, while overseen by federal, state, and/or municipal authorities.
It's important to note that while standards aren't mandated by law, many regulatory authorities recognize standards and recommend adherence to them in order to promote safety and quality.
What kind of standards are medtech manufacturers responsible for tracking?
The medical device industry has the responsibility for the design and manufacturing of a wide range of products used to diagnose and treat illnesses to improve health in patients. Medical device standards help ensure that a manufacturing or design process can consistently produce the quality required to serve patients and healthcare professionals around the world.
Some of the more common standards used by the medtech industry include, but are certainly not limited to:
ISO 9001 – A general standard (not industry specific) for quality management and implementing a rigorous quality system. For medtech specifically, it helps with the management of the quality control process by helping to keep costs low, improve accountability and simplify regulatory compliance.
ISO 13485 – This standard is designed for medtech specifically and expands on the framework set up by ISO 9001. Compliance with this standard helps with quality control, process validation, and risk management, often referred to as the risk management standard.
ISO 14971 – This standard specifies terminology, principles, and a process for the risk management of medical devices, including software and in vitro. This helps to identify hazards that may be associated with devices and to minimize those risks.
IEC 60601-1 – Medical Electrical Equipment, general requirements for basic safety and essential performance of equipment.
ISO 10993 – Biological evaluation of medical devices that includes biocompatibility testing of materials used to design product parts that would come into contact with a patient, testing for skin sensitization, and irritabilities.
ISO 15223 – Symbols to be used with information to be supplied by the manufacturer. This standard identifies symbols that are globally accepted to be used in a broad spectrum of medical devices. These symbols can be placed on the device, on the packaging, or on any accompanying information such as instructions for use.
ISO 45001 – This standard outlines the requirements for occupational health and safety management systems that can be employed in the medical device industry to help reduce occupational risk.
Where do I get these standards?
Standards used to design and build medical devices need to be purchased, and you must always maintain the most current revision of that standard to ensure proper adherence to it. They can be purchased as electronic copies, or you can request a paper copy for your files. You can purchase them directly from the standard organization (ISO, IEC, ASTM, UL, etc.). There are also organizations services that will provide standards from many organizations, serving as your to be your one-stop shop.
How do I know when standards change?
The best way to manage how you receive information about changes to industry standards would be to implement an electronic standard tracking system. These systems help to:
- Give you early notifications of changes
- Mitigate your company's risk by ensuring you're up-to-date
- Save you time by eliminating the tracking on your own
- Ensure your standards are up-to-date
Using manual processes such as spreadsheets to manage standards updates can be difficult, time-consuming, and lead to compliance risks - especially when a high number of standards and markets are involved. There are a variety of standards management tools to help medtech companies monitor and manage global standards, including Rimsys.
How can Rimsys help?
Rimsys’ regulatory management software offers standards management to help you stay ahead of the mayhem by providing:
- Access to a library of over 1.6 million global standards through a partnership with IHS Markit
- The ability to link standards to individual products to more easily assess the impact of changes across your product portfolio
- Automatic alerts when standards are changed, superseded, or withdrawn to reduce compliance risks and enable faster reaction times
- Bulk updates to your essential principles/GSPR tables when standards change for easier maintenance and compliance
For more information, visit www.rimsys.io/solutions/standards-management.

Why should you invest in your regulatory team? Easy Medical Device podcast interview
Recently, our Founder and CEO, James Gianoutsos, was a guest on an episode of the Easy Medical Device podcast. Hosted by Monir El Azzouzi, a quality and regulatory professional with over 16 years of industry experience, the Easy Medical Device podcast explores a wide range of topics, news, and challenges to help medtech quality and regulatory professionals gain valuable insights that will help them excel in their roles.
In the episode, Why should you invest in your regulatory team?, James and Monir explore the limitations of traditional cost-center approaches to resourcing and preparing budgets for regulatory affairs teams and discuss the benefits of treating regulatory affairs as a revenue function. Hear their thoughts about:
- How regulatory affiars teams are typically structured
- The importance of the RA job function on revenue
- The impact AI will have on regulatory affairs
- How digital tools can enable RA teams
James also provided tips RA professionals can use to convince their stakeholders to invest in regulatory affairs teams. He emphasized that getting buy-in often involves a mindset shift that will change the dynamic of the conversation. For example, when planning for a renewal, think about the financial impacts of missed renewals rather than the sheer volume of renewals you're doing.
When you're trying to convince your leadership team, don't talk about how many renewals I did for this product in a particular month. talk about the dollar figures you saved the company or retained on the market.
For more tips, listen to the full interview on the Easy Medical Device website.
Taking SaMDs to market in the US: How is the FDA regulating adaptive machine learning algorithms?
Rimsys recently held a panel discussion, Taking SaMDs to market in the US. During it, Prabhu Raghavan, Principal at MDQR Solutions, and Rimsys Chief Solutions Officer, Brad Ryba, shared an overview of SaMDs and provided their insights about getting and maintaining market clearance for them in the United States. Topics ranged from FDA risk classifications and submissions, cybersecurity best practices, and machine learning algorithms, which brought about an important question: How is the FDA currently regulating adaptive machine learning algorithms in SaMDS?
Adaptive machine learning algorithms use post-market data in real time and evolve their models based on the data they're consuming. As such, every patient utilizing a device with adaptive machine learning algorithms may have a new model compared to the previous patient. While the FDA doesn't have any formal guidance on the subject just yet, manufacturers can work with the FDA to get a plan in place for maintaining a state of validation post market.
Watch the snippet from the webinar to learn about taking a staged approach with the FDA to get a proper validation plan in place.
To watch all discussion topics, download the webinar replay here.

The five guiding principles for machine learning-enabled medical devices using PCCPs
On October 24th, 2023, the FDA, Health Canada, and the MHRA published a joint document providing harmonization for machine learning-enabled medical devices (MLMD) that use predetermined change control plans (PCCPs). PCCPs are plans proposed by the manufacturer that state the specific modifications to a MLMD, the process for implementing these modifications, and the assessment of impacts from them.
The document details five guiding principles for MLMDs in an effort to set a foundation for PCCPs and encourage collaboration on them. According to the UK government’s website, these principles are:
- Focused and Bounded: Describing specific changes that a manufacturer intends to implement.
- Risk-based: The intent, design, and implementation of a PCCP are driven by a risk-based approach that adheres to the principles of risk management.
- Evidence-based: Demonstrating that benefits outweigh the risks throughout the product lifecycle.
- Transparent: Provide clear and appropriate information and detailed plans for ongoing transparency to all stakeholders, from patients to healthcare professionals.
- Total Product Lifecycle Perspective: Improve the quality and integrity of a PCCP by continually considering the perspectives of all stakeholders.
Here are some examples of how these principles could be applied:
- Focused and bounded: A manufacturer of an MLMD that diagnoses cancer might develop a PCCP to implement a change to the algorithm that improves its accuracy in detecting a specific type of cancer.
- Risk-based: A manufacturer of an MLMD that monitors a patient's vital signs might develop a PCCP to implement a change to the algorithm that reduces the likelihood of false alarms.
- Evidence-based: A manufacturer of an MLMD that delivers medication to patients might develop a PCCP to implement a change to the algorithm that improves the accuracy of the dosage.
- Transparent: A manufacturer of an MLMD might publish a white paper that describes the device's algorithm and how it was developed and tested. The manufacturer might also make available a user manual that provides clear instructions on how to use the device safely and effectively.
- Total product lifecycle perspective: A manufacturer of an MLMD might collect feedback from patients and healthcare professionals on how the device is performing after it is marketed. The manufacturer might also use this feedback to identify and address any potential problems with the device.
The five guiding principles for MLMDs using PCCPs are based on the 10 guiding principles for Good Machine Learning Practices (GMLP) published in 2021, which were designed to help medical device manufacturers develop and deploy machine learning models that are safe, effective, and high quality. Similarly, the goal of these five guiding principles is to help MLMD manufacturers develop and maintain safe and effective products that meet the needs of patients and healthcare professionals. They are also intended to streamline the regulatory process for MLMDs, making it easier for manufacturers to bring new products to market and make updates to existing products in a timely manner.
If you’re looking for additional information about MLMD requirements in the US, join Rimsys and MDQR Solutions for Taking SaMDs to market in the US on Thursday, November 30th, at 1 PM ET. We’ll discuss the various types of SaMDs, considerations to make when obtaining market clearance, and how the FDA is regulating AI/ML in devices. Those interested in attending can register here: Taking SaMDs to market in the US.
