


Featured
Rimsys Announces Rimsys AI to Eliminate Repetitive Tasks and Enhance Decision-Making for MedTech Regulatory Teams
Rimsys, the leading Regulatory Information Management (RIM) platform for the MedTech industry, today announced the launch of Rimsys AI, a suite of embedded artificial intelligence (AI) agents.

The ultimate guide to the medical device single audit program (MDSAP)
This article is an excerpt from The ultimate guide to the medical device single audit program (MDSAP) ebook.
Table of contents
- What is MDSAP?
- History of MDSAP
- Who is responsible for the MDSAP?
- How does an MDSAP audit work?
- Audit sequence
- You got a nonconformity – now what?
- What does an MDSAP audit cost?
- Why choose the MDSAP certification process?
- Potential disadvantages of the MDSAP
- Ready to participate? – Here’s how to get started
- Completing a successful MDSAP audit
The Medical Device Single Audit Program (MDSAP) was designed and developed to allow a single audit of a medical device manufacturer to be applied to all country markets whose regulatory authorities are members of the program. The MDSAP provides efficient and thorough coverage of the standard requirements for medical device manufacturer quality management systems, and requirements for regulatory purposes (ISO 13485:2016). In addition, there are specific requirements of each medical device regulatory authority participating in the MDSAP that must be met:
- Conformity Assessment Procedures of the Australian Therapeutic Goods (Medical Devices) Regulations (TG(MD)R Sch3)
- Brazilian Good Manufacturing Practices (RDC ANVISA 16)
- Medical Device Regulations of Health Canada (ISO 13485:2003)
- Japan Ordinance on Standards for Manufacturing Control and Quality Control of Medical Devices and In Vitro Diagnostic Reagents (MHLW Ministerial Ordinance No 169)
- Quality System Regulation (21 CFR Part 820), and specific requirements of medical device regulatory authorities participating in the MDSAP program.
This means that a report from a single MDSAP audit of a medical device manufacturer would be accepted as a substitute for routine inspections by all the member Regulatory Authorities (RAs) across the world. There are currently five participating Regulatory Authorities (RA) representing the following countries: Australia, Brazil, Canada, Japan and the USA.

In April, 2021, the RAs released an “Audit Approach” document (MDSAP AU P0002.006) that combines the formerly separate MDSAP Audit Model and Process Companion documents into a single guidance document. It includes guidance for assessing the conformity of each process and includes an audit sequence, instructions for auditing each specific process, and identifies links that highlight the interactions between the processes.
In March 2012 the US FDA announced that they had approved a final pilot guidance document “Guidance for Industry, Third Parties and Food and Drug Administration Staff: Medical Device ISO 13485:2003 Voluntary Audit Report Submission Pilot Program.” This allowed the owner or operator of a medical device manufacturing facility to be removed from FDA’s routine inspection work plan for 1 year upon completing a ISO 13485:2003 audit. This guidance document went into effect in June 2012, and was intended as an interim measure while a single audit program was being developed.
This pilot program was not very successful and few companies signed up because they did not see any advantage in participating. The manufacturer had to pay for a third party to inspect their facilities, generate a report, and share the inspection results back to the FDA. Many companies were reluctant to contract “someone else” to perform their inspection when they could easily wait for the FDA to conduct an inspection for free.
During its inaugural meeting in Singapore in 2012, the International Medical Device Regulators Forum (IMDRF) appointed a working group to develop a set of documents for a harmonized third-party auditor system. Hence, the “Medical Device Single Audit Program” (MDSAP) was formed. The concept was similar to the FDA’s original idea of creating a third-party auditor to help reduce their workload of performing regulatory audits of medical device manufacturers’ quality management systems. This new approach would consist of a single audit that would review regulatory QMS compliance, conducted by a third-party, who would later be called an Auditing Organization (AO).
From January 2014 to December 2016, five countries participated in a Medical Device Single Audit Program Pilot. In June 2017, a report was generated summarizing the outcomes of prospective “proof- of-concept” criteria established to confirm the success of the program. The outcomes are documented in the final MDSAP Pilot Report and recommended that the program become fully active and open to any manufacturer who requested this type of audit.
The governing body of the MDSAP is the Regulatory Authority Council (RAC), which is composed of two senior managers (and a few other staff members) from each participating RA. They are responsible for executive planning, strategic priorities, setting policy, and making decisions on behalf of the MDSAP International Consortium. The RAC also reviews and approves documents, procedures, work instructions, and more. The mission of the MDSAP International Consortium is to jointly leverage regulatory resources to manage an efficient, effective, and sustainable single audit program focused on the oversight of medical device manufacturers on a global scale.
Other international partners that are involved in the MDSAP include:
MDSAP Observers:
- European Union (EU)
- United Kingdom’s Medicines and Healthcare products Regulatory Agency (MHRA)
- The World Health Organization (WHO) Prequalification of In Vitro Diagnostics (IVDs) Program
MDSAP Affiliate Members:
- Argentina’s National Administration of Drugs, Foods and Medical Devices (ANMAT)
- Republic of Korea’s Ministry of Food and Drug Safety
- Singapore’s Health Sciences Authority (HSA)
The observers and affiliate members are not the same as the participating member RA’s. The observers simply observe and/or contribute to RAC activities. Affiliate members, on the other hand, are interested in engaging in the MDSAP program and are subject to certain rules. They are only given access to a certain level of information about the manufacturers, audit dates, and information in audit reports.
They are also invited to attend sessions that are open to members, observers, and affiliates only.
Audits can also be conducted by MDSAP participating RAs at any time and for various reasons including:
- "For Cause" due to information obtained by the regulatory authority
- as a follow up to findings from a previous audit
- to confirm the effective implementation of the MDSAP requirements
The purpose of audits conducted by the RAs is to ensure appropriate oversight of the AOs MDSAP auditing activities. The AOs are appointed by the RAs and a list of the currently approved AO’s is published on the FDA website. Most AOs offer a broad range of management system certification services, beyond just medical devices. Manufacturers should verify that prospective AOs are clearly trained and perform MDSAP audits of medical devices.
AOs have the final word as to whether a manufacturer has met the requirements for the MDSAP during the execution of the audit and generation of the associated reports summarizing the results. MSDAP RAC participating RAs have the final decision regarding all development, implementation, maintenance, and expansion activities associated with the program.
Although an unannounced visit by an AO is rare, it can happen in circumstances where high-grade nonconformities have been detected.
To continue reading this eBook including a detailed look at the MDSAP audit process and grading, pros and cons of the approach, and how to get started please register to download the full version.
The beginner's guide to the FDA 510(k)
This article is an excerpt from The beginner's guide to the 510(k) ebook.
Table of Contents
- Introduction
- 510(k) basics
- Contents of a Traditional 510(k)
- 510(k) submission and timelines
- Other 510(k) forms
Congratulations! You have successfully developed a new medical device. Now you need to take it to market. In the United States, this often means submitting a 510(k). A 510(k) is a structured package of information about your device and its performance and safety that you submit to the Food and Drug Administration (FDA) for “clearance” before you can sell your device in the U.S. In order to receive clearance from the FDA, your 510(k) will need to demonstrate that your medical device is substantially equivalent to another legally marketed device (called a predicate device). The substantial equivalence approval process is a simple equation that looks something like this:

The 510(k) is generally the most efficient route to market clearance in the U.S. because you show your device is safe and effective based on this substantial equivalence standard, instead of needing to present more extensive clinical trial data.
There are three types of 510(k): Traditional, Abbreviated, and Special. This eBook will begin with a general overview of the 510(k) process, including its purpose and benefits. Next, we will explore the Traditional 510(k) and the sections and components required in depth. Finally, we will look at the Special and Abbreviated 510(k).
FDA: background and device oversight
Before we explain what a 510(k) is let’s first talk generally about the FDA and device oversight. The FDA is the U.S. governmental agency responsible for overseeing medical devices, drugs, food, and tobacco products. When it comes to medical devices, the FDA’s mission is to “protect the public health by ensuring the safety, efficacy, and security of…medical devices.” At the same time, the FDA also has an interest in “advancing public health by helping to speed innovations.” In other words, the FDA’s goal is to make sure devices are safe and effective for public use, while also ensuring that devices have a quick and efficient path to market.
In order to achieve this balance of safety and efficiency, the FDA has three different levels of oversight depending on the risk level of the device: (1) exempt from premarket submission, (2) Premarket Notification, also known as 510(k), and (3) Premarket Approval (PMA).
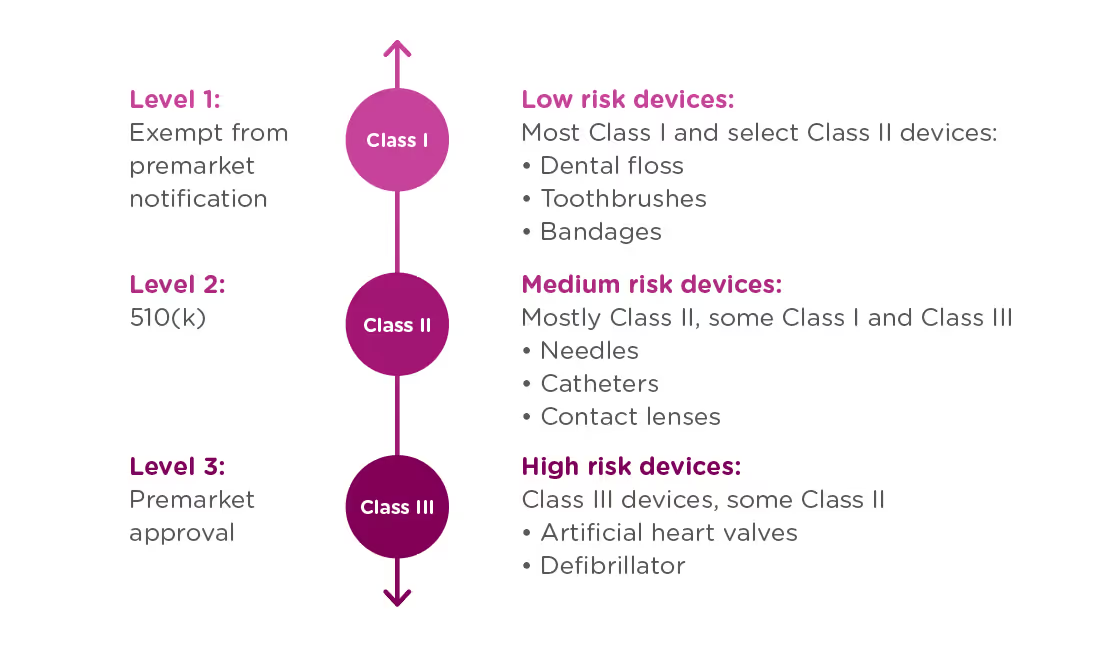
When is a 510(k) required?
A 510(k) is required for medium risk devices that have a predicate on the market which can be used to demonstrate the safety and effectiveness of the new device. Meanwhile, a PMA is required for high-risk or novel devices which require a higher level of scrutiny to be confirmed safe and effective.
A 510(k) is not only required for new devices, but also for devices that have been modified in a way that could impact safety or effectiveness. This could include changes to the:
- Design
- Components
- Materials
- Chemical composition
- Energy source
- Manufacturing process
- Intended use
You must submit your 510(k) at least 90 days before marketing the device.
What Exactly is Substantial Equivalence?
Now that we know what a 510(k) is, let’s talk about the substantial equivalence standard. You’ll recall from the introduction that your 510(k) must show that the new (or modified) device is substantially equivalent to at least one other legally marketed device, called a predicate device. Substantial equivalence looks at the intended use and the technological characteristics of the two devices.
More specifically, you must show:
- that the new device has the same intended use as the predicate, and
- the differences between the two devices do not raise questions about the safety and effectiveness of the new device.
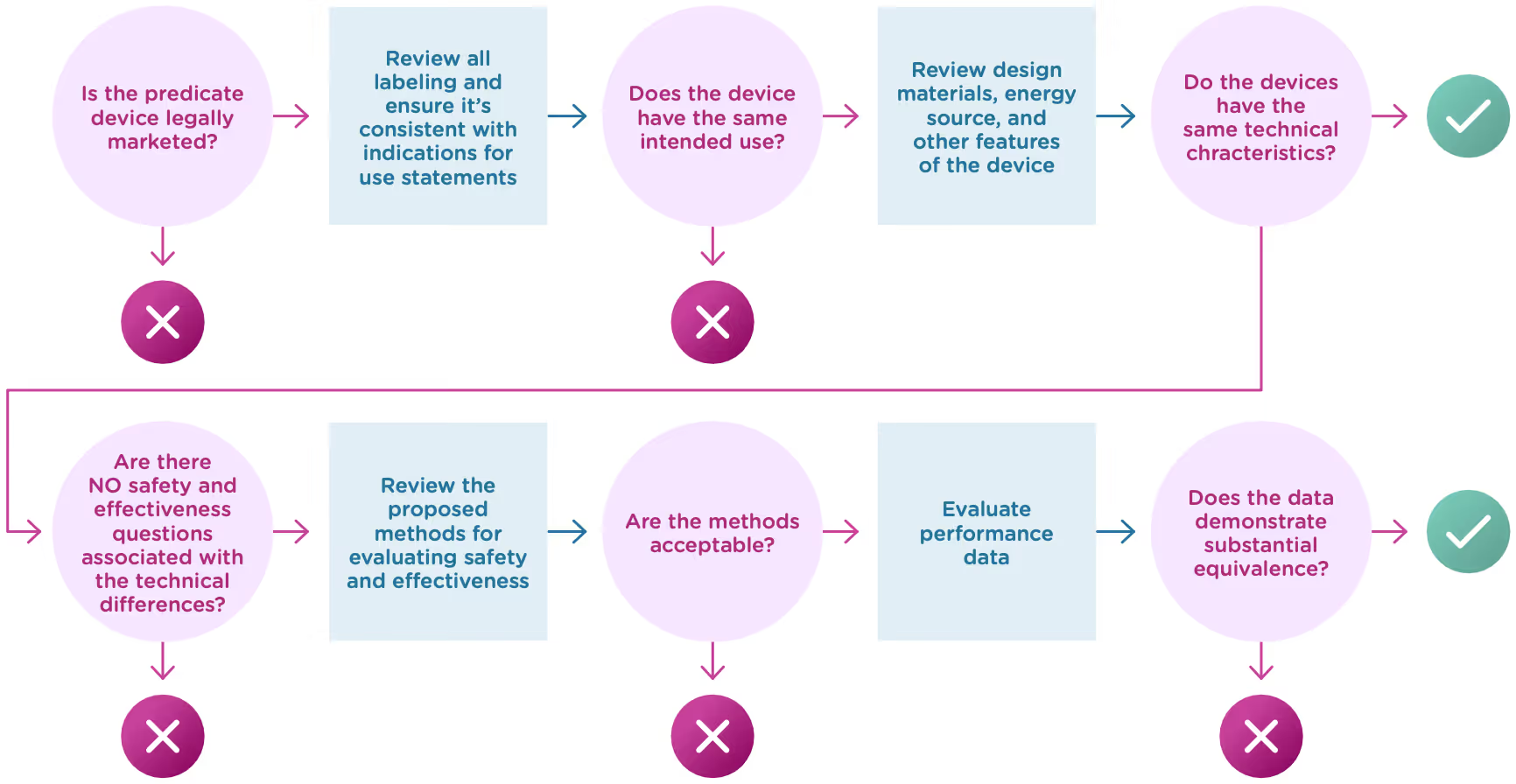
Now let’s take a closer look at intended use and technological characteristics.
Intended use
Intended use means the general purpose or function of the device. The FDA will look at your proposed labelling and your Indications of Use section of the 510(k) to determine the intended use of your device (this is covered in Chapter 2). Intended use includes:

Technological characteristics
Once the FDA has determined that a predicate device exists and that the new device and the predicate device have the same intended use, it will move on to compare the technological characteristics. Technological characteristics include:
- Materials
- Design
- Energy source
- Other device features
The two devices do not have to be identical, and in fact they almost never are. The key here is to demonstrate that any differences do not have a significant impact on safety or effectiveness. Here’s what to cover when you compare your device’s technological characteristics with that of the predicate device:
Overall description of the device design
- Engineering drawings or diagrams to explain the device and component parts.
- List of component parts and explanation of how each component contributes to the overall use and function of the device.
- Physical specifications: dimensions, weight, temperature, tolerances, etc.
Materials
- Detailed chemical formulation used in all materials of constructions (especially those that come into contact with a patient).
- Any additives, coatings, paint, or surface modifications.
- How materials have been processed and what state they’re in.
Energy Sources
- Use of batteries, electricity, etc.
Other technological features
- Software/hardware
- Features
- Density
- Porosity
- Degradation characteristics
- Nature of reagents
- Principle of the assay method
In deciding whether the differences in technological characteristics impact safety or effectiveness, the FDA will typically rely on descriptive information about the technological characteristics as well as non-clinical and clinical performance data.
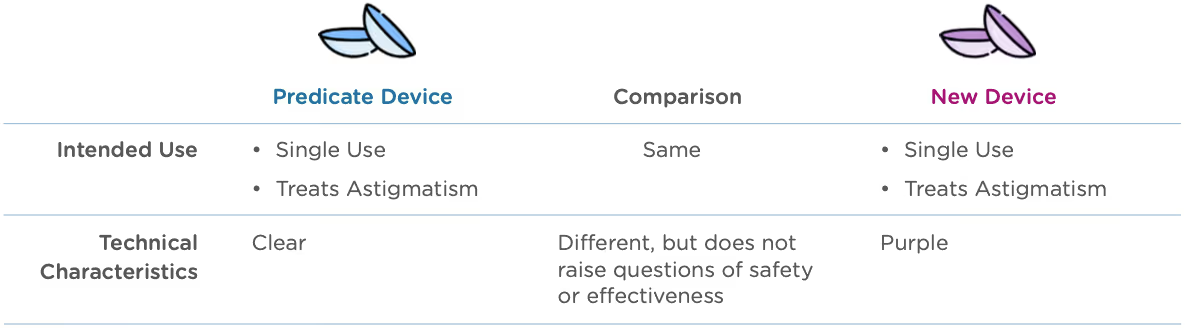
Let’s look at an example: A manufacturer submits a 510(k) for a new type of contact lens. Both the new device and the predicate device are indicated for daily wear for the treatment of astigmatism. The predicate device is only available in a clear lens, but the new device comes in a line of colors, including purple tinted lenses.
Who is responsible for submitting a 510(k)?
The following four types of organizations may be responsible for submitting a 510(k):
Manufacturers
- End-of-line device manufacturers who will be placing a device on the U.S. market.
- Note: Does not apply to component part manufacturers unless components will be marketed independently.
Specification developers
- Companies that develop the specifications for a finished device which has been manufactured elsewhere
Repackers or relabelers
- Required to submit a 510(k) if they significantly alter the labeling or condition of the device, including modification of manuals, changing the intended use, deleting or adding warnings, contraindications, sterilization status.
- Note: This is rare. The manufacturer, not the repackager or labeler, is typically responsible for the 510(k) submission.
Importers
- Importers that introduce a new device to the U.S. market may need to submit a 510(k), if it hasn’t already been submitted by the manufacturer.
Now that we’ve covered the basics, let’s explore what actually goes into your 510(k).
A Traditional 510(k) should contain all the following components in the list below. In some cases, a particular section may not apply to your device. When that happens, it’s a good idea to include the section anyway and just state “This section does not apply” or “N/A” under that heading.
To continue reading this eBook including a detailed walk-through of all the Traditional 510(k) components, submission requirements and timelines, and an overview of the other 510(k) forms including the Abbreviated 510(k) and the Special 510(k), please register to download the full version


The ultimate guide to the China UDI system and database
This article is an excerpt from The ultimate guide to the China NMPA UDI system and database ebook.
Table of Contents
- Overview
- UDI basics and benefits
- UDI format requirements and issuing entities
- UDI database and submission requirements
- Implementation of UDI and the UDI database in China
The current Chinese medical device regulatory regime kicked-off in 2014 with the Regulation on Supervision and Administration of Medical Devices. This core set of registration requirements, modeled after the United States and European Union systems, established a set of device classifications (class I, II, and III) based on risk and procedures for obtaining market clearance for each type of device.
Medical devices in China are regulated by the National Medical Products Administration (NMPA). Class I devices, such as clinical laboratory equipment or non-invasive skin dressings, require only notification to the NMPA for marketing authorization, and that authorization does not expire. Class II and III devices such as implantable devices or devices with a measuring function require full registration and a formal review before market clearance can be obtained.
These initial regulations have been expanded since their introduction, adding accelerated pathways to market for certain products in certain regions, easing acceptance of clinical data from overseas, and more specific roles and responsibilities for local agents of international manufacturers. In addition, in 2019, the regulations added a provision that medical devices carry a unique device identification (UDI). China’s UDI requirements are similar to those in the US and European Union. They establish specific device ID and labeling requirements, as well as a central, state-administered database of devices.
This eBook walks through the basics of medical device UDIs, the specifics of China’s implementation, and how MedTech companies who market their devices in China can prepare for the full rollout of these regulations in the coming years.
A UDI is a unique alphanumeric code that is designed to identify medical devices sold in a particular country/region from manufacturing, through distribution, to use by a patient. Like other aspects of the medical device regulatory regime, the UDI system in China follows the approach taken by the United States FDA and European Commission, and is based on the guidance from the International Medical Device Regulators Forum (IMDRF). Generally, UDI systems are designed to improve patient safety and optimize care by:
- Increasing the traceability of medical devices, including field safety corrective actions
- Providing an unambiguous identification method for medical devices throughout distribution and use
- Making adverse event reports more accessible
- Reducing medical errors by providing detailed information related to the device
- Simplifying medical device documentation and making it more consistent
There are three components to the UDI system in China:
- UDI code: The actual UDI code can be assigned by one of three (3) issuing agencies and contains information about the product, it’s expiration date, and the manufacturing batch/lot it’s associated with.
- UDI labeling: Put simply, medical devices must carry the UDI code on them. The regulations stipulate how devices and their packaging must be labeled for compliance.
- UDI database: In addition to labeling, all device UDIs must be submitted to a central database that is administered by the NMPA.
The following sections explore each of these components in more detail.
The UDI code
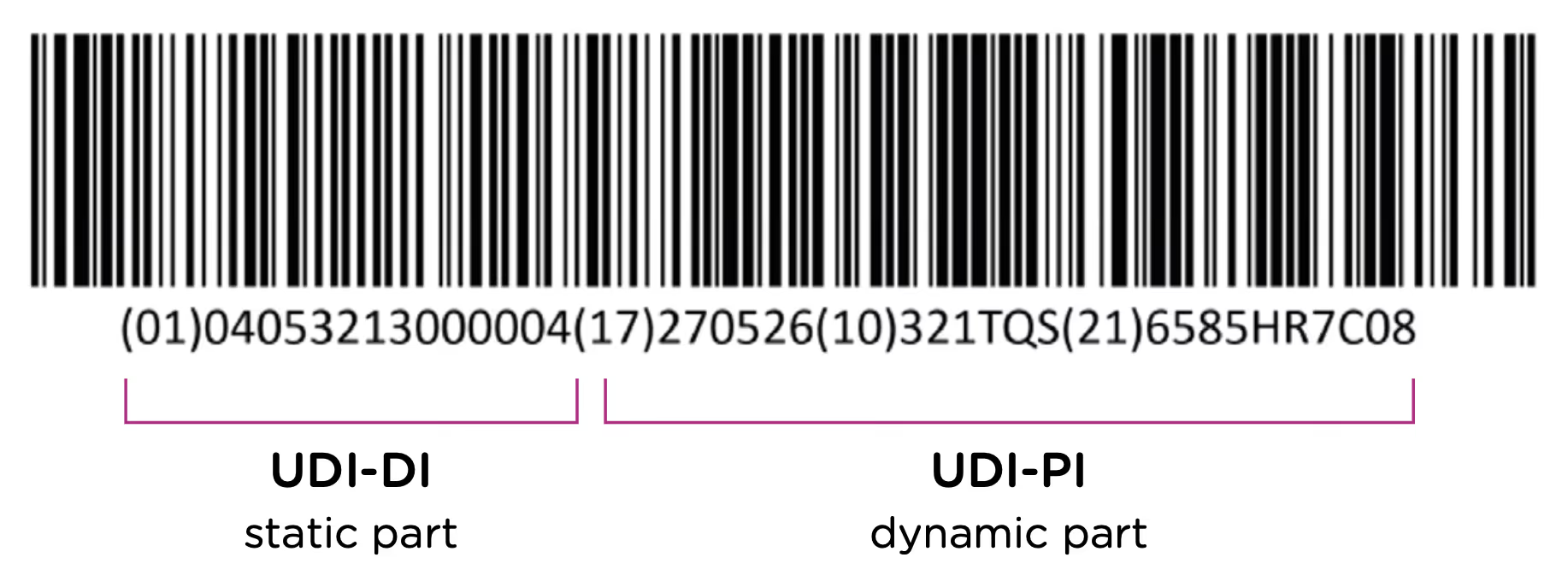
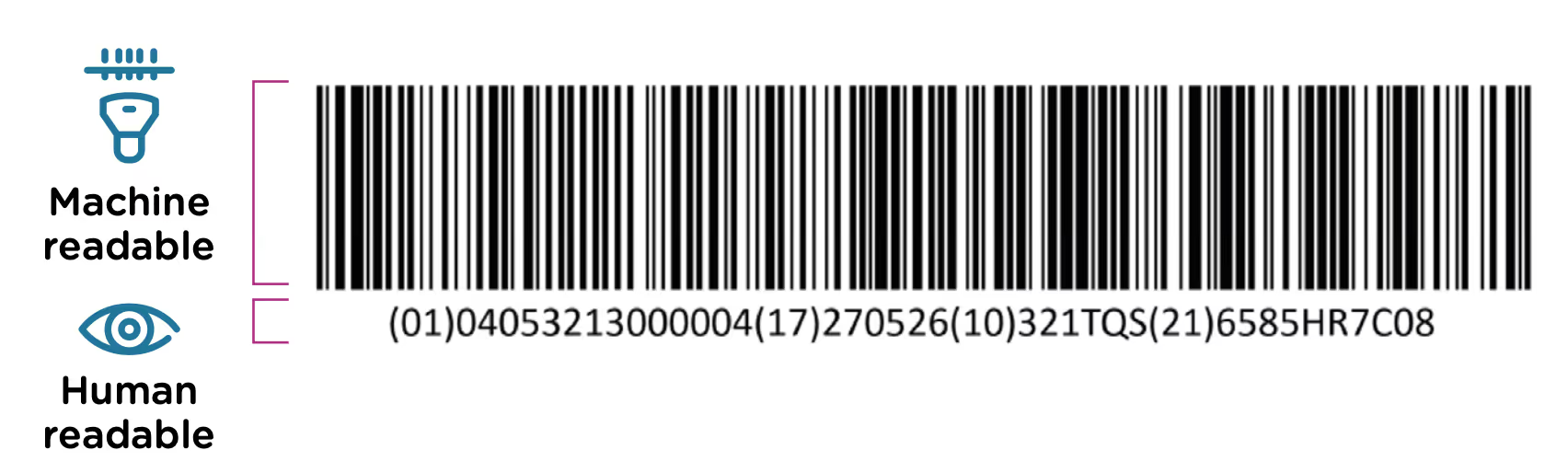
The first element of the UDI system is the code itself. The UDI code is the alphanumeric identifier that is associated with a specific medical device. UDI codes have two (2) elements to them, the UDI device identifier (UDI-DI) or static portion, and the UDI production identifier (UDI-PI) or dynamic portion. You can see the two components in the UDI diagram below:
The UDI-DI contains information about the issuing entity—the organization that is authorized to assign UDI codes. In China, this can be one of three entities: GS1, an international barcode and electronic data interchange standards organization, and two domestic organizations: the Zhongguancun Industry & Information Research Institute (ZIIOT), and AliHealth. Additional details about the issuing agencies are covered in Chapter 2. In addition, the UDI-DI contains information about the manufacturer and the specific model or version of the device.
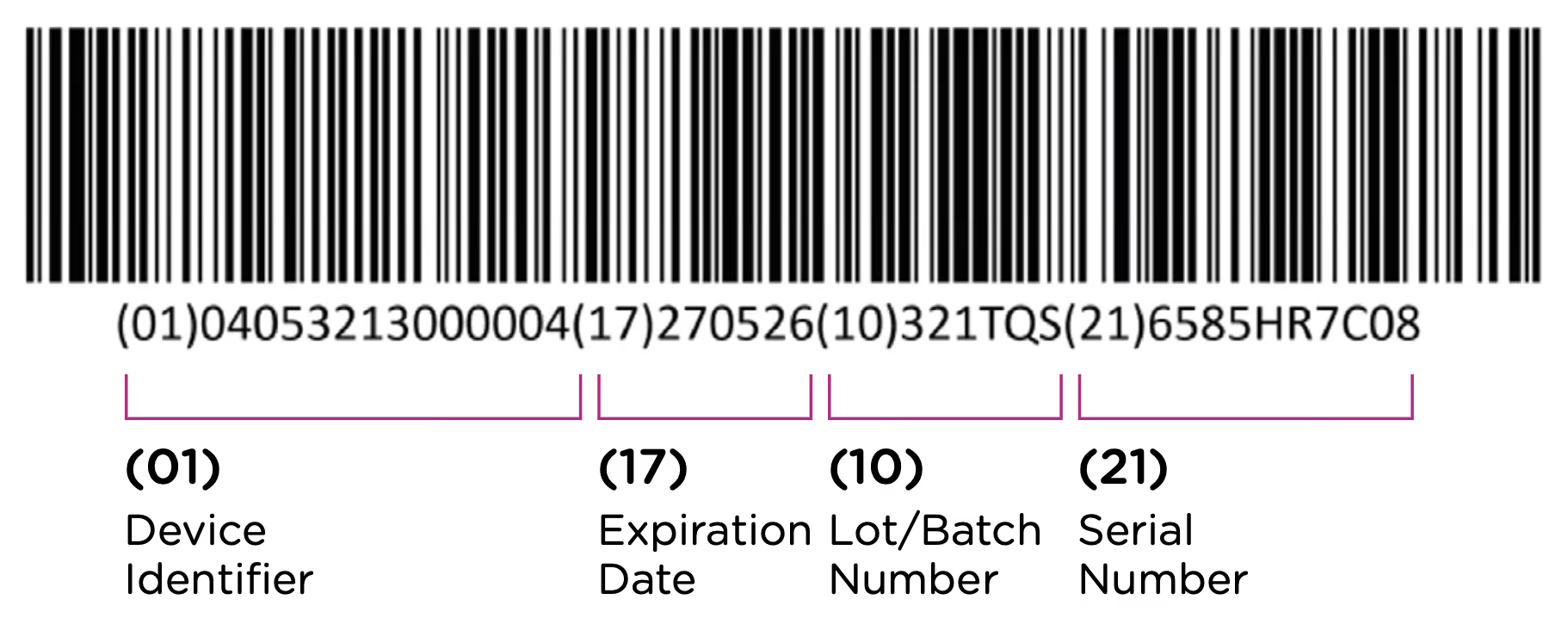
The UDI-PI contains information about the manufacturing and production of the device. This typically includes information about the lot or batch number in which the device was manufactured, the manufacturing date and expiration date for the device (if applicable), and the specific serial number for the device. Here you can see all of the components marked up using the same UDI example:
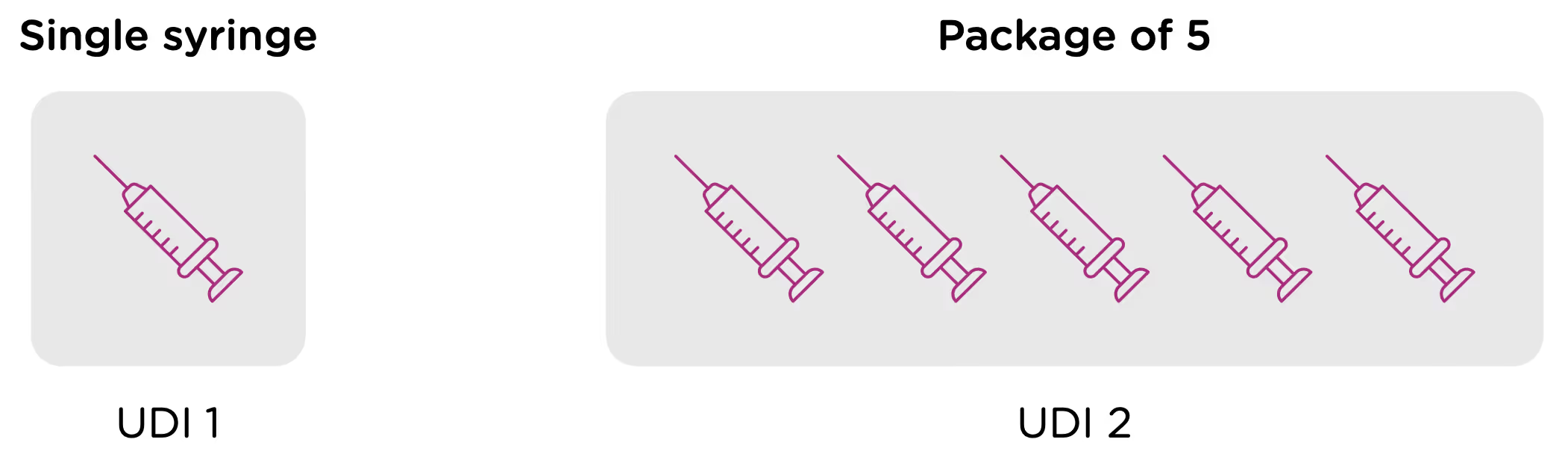
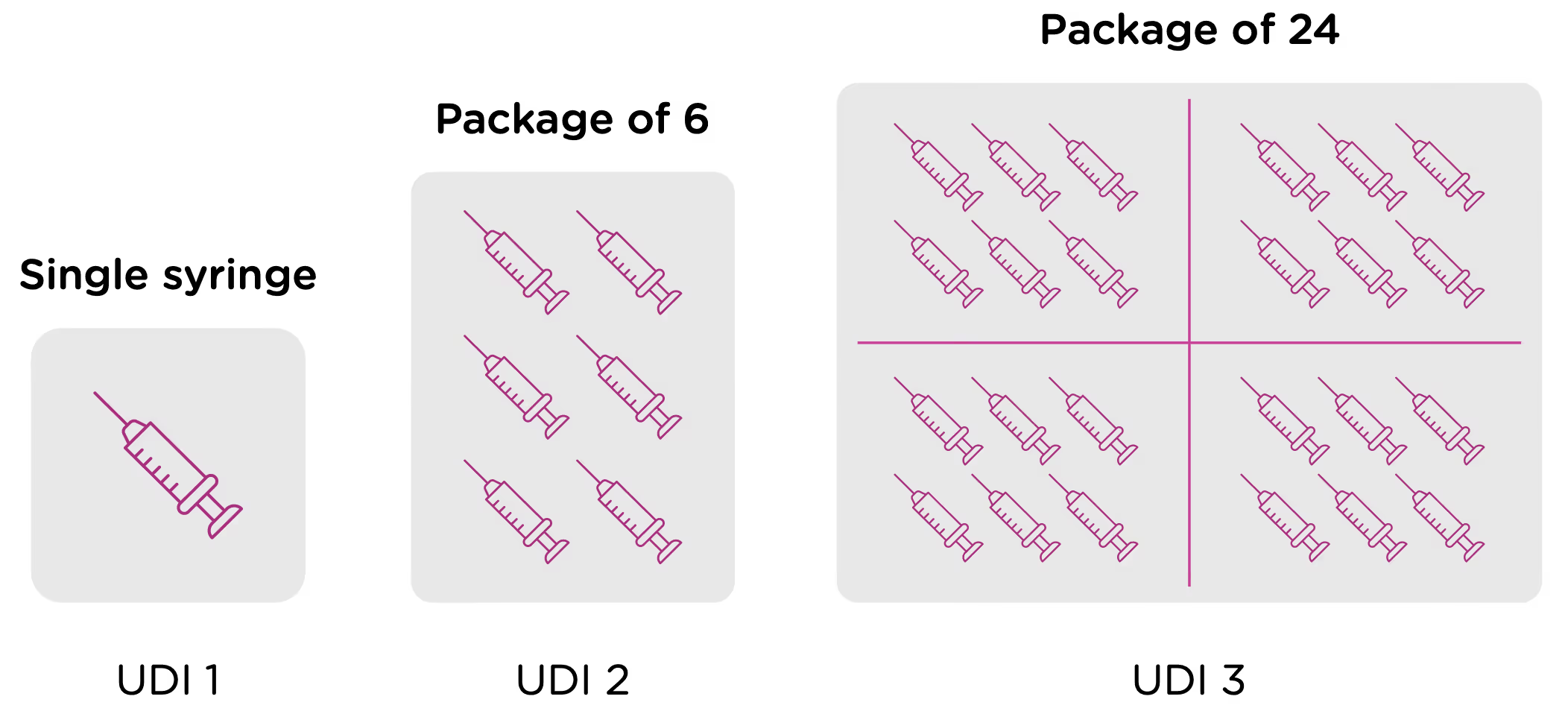
Note that each packaging permutation and level for a given device will need to be assigned its own UDI. So for example, let’s say that a company manufactures 5ml enteral (oral) syringes in two packaging options: 1 – packaged individually and 2 – packaged in a box of 5. Each packaging option would need its own UDI, despite the fact that the underlying product is the same.
Now looking at packaging levels, let’s assume that the manufacturer packages the single syringe offering into boxes of 6, and again into larger containers of 24. Each of those packaging options needs its own UDI as well.
Labeling
In addition to obtaining UDI code for each device as outlined in the previous section, medical device manufacturers are required to ensure that devices are appropriately labeled with the assigned UDI. This label is called the UDI Carrier. The UDI is represented in two forms on the UDI Carrier: a machine-readable form and a human-readable form.
The machine-readable form or automatic identification data capture (AIDC) is a barcode or some other technology that can be used to automatically capture UDI information. The NMPA regulations support 3 types of machine-readable formats: 1-dimensional barcode, 2-dimensional barcode, and radio-frequency identification (RFID).

The regulations note that “use of advanced automatic identification and data collection technologies is encouraged”—prompting manufacturers to use more modern 2D and RFID machine-readable carriers where possible. Note, however, that if a device uses RFID, the UDI Carrier must also include the UDI in barcode format.
The human-readable form or human-readable interpretation (HRI) is the numeric or alphanumeric code for the UDI that can be read and manually entered into systems.
The UDI Carrier should be included on the device and on all levels of packaging. The UDI Carrier must be clear and readable during the operation and use of devices. If there isn’t room on the device for both the human and machine-readable forms of the UDI, then manufacturers should prioritize the machine-readable form.
UDI database
The third component of the NMPA UDI system is the UDI database. This is a centralized database of UDI and product information, administered by the NMPA. Manufacturers are required to submit UDI information into the database within 60 days after a product is approved (for sale in China) and before it is commercialized. The database contains a more detailed product record than what is included in the UDI itself, and it is the responsibility of the manufacturer (and/or their in-country representative) to submit the information correctly, and ensure that it’s kept up to date.
Chapter 3 of this eBook goes into detail about the specific fields and data requirements for UDI database submissions.
To continue reading this eBook including information about UDI format requirements and issuing entities, implementation timelines, and affected device types, please register to download the full version.


SaaS 101 for medtech regulatory professionals
What is Software as a Service (SaaS)?
SaaS, or Software as a Service, is a software delivery model in which applications are hosted by software vendors and provided to users via the internet. The use of SaaS software has skyrocketed in recent years, with an estimated 70% of business software being used falling into the SaaS category 2022.
Also known as a “cloud” delivery model, SaaS solution providers either host the application and related data using their own servers and computing resources or use a cloud service provider, such as Amazon Web Services (AWS) or Microsoft Azure, to host the application in the provider's data center. The hosted application is then accessible to any device with a network connection and is usually accessed via a web browser.
Many SaaS software systems use a multi-tenant architecture in which a single instance of the software serves many subscribers, or users. Customer data, while stored centrally, is logically separated to ensure security and prevent co-mingling of data. However, for software systems that require validation, such as regulatory information management systems, a single-tenant system can offer greater data security along with the flexibility for teams to fully validate software releases before adopting them.
What are the benefits of Saas?
- Reduced hardware costs – SaaS removes the need to install and maintain software locally, which reduces the cost of servers and related infrastructure.
- Subscription payments – SaaS software is typically billed on a monthly or annual subscription basis. Not only does this allow companies to spread out the cost of the system, but a subscription model also allows for shorter commitment periods vs. a large up-front capital expenditure (CapEx vs OpEx). The SaaS model also holds software providers more accountable than other models given that the user has the option to cancel or not renew a SaaS subscription, leading to higher levels of service and support.
- Scalable usage – SaaS service providers automatically scale the resources needed to support users and can provide additional services or features on demand.
- Seamless software maintenance – SaaS software can be automatically updated with new features and, when necessary, patched with bug fixes. While this simplifies software maintenance from the user’s end, users in the medtech industry should expect to be able to test and validate software updates before they are installed on their system.
- Accessibility – Accessed via the Internet, SaaS solutions are available from almost any device in any location.
- Reliability – Because SaaS solution providers have extensive resources, beyond what any individual company would normally have, SaaS software typically has very high reliability and availability in comparison to in-house systems.
- Security – SaaS solution providers deliver state-of-the-art security and privacy at a level that is difficult for individual companies to maintain.
As a regulatory professional, what questions should I ask a SaaS vendor?
How are software updates managed?
SaaS software providers generally install new features, bug fixes, and other updates automatically. However, medical device regulations, such as the FDA’s 21CFR Part 11 and EU’s MDR, require medtech companies to validate any software that they are using that is integral to their quality system or otherwise might affect the safety or efficacy of the devices which they manufacture.
Therefore, a SaaS company providing solutions to the medtech industry should offer the ability for subscribers to review and validate software updates before they are installed. This is often done by providing a transition period during which the software vendor allows access to the new version of the software and the existing version. In addition, many software providers, such as Rimsys, will turn off new features by default and allow the user to enable the new feature if and when they want to begin using it. Be sure to understand what, if any, updates will be installed without this review period. Some software vendors will push small bug fixes and minor features automatically.
Clients should be notified of any updates in a timely manner and, ideally, have access to a non-production version of the software for testing purposes. Be sure to understand how often updates will become available and how often those updates are expected to trigger a re-validation of the system. While every medtech organization will have their own specific policies on this matter, Rimsys communicates the expected impact on software validation of each new release, and the reasoning behind whether an update will or will not require a new validation.
Do you assist with software validation?
While software validation is ultimately the responsibility of the medtech company using the software, there is a lot that a software vendor can do to assist with this process. The software vendor should be able to provide documentation concerning the design, development, and testing of the systems that they are providing. In addition, some vendors will provide test cases that can be used by your own team to test and validate the software. These test cases significantly reduce the burden on the in-house validation team.
SaaS vendors should also be able to provide medtech companies with their Computer Software Assurance (CSA) plan. In most cases, the FDA and similar regulatory agencies are looking for compliance with a CSA plan in lieu of the more onerous Computer System Validation (CSV) process that was traditionally followed in the past.
How do you handle data security?
This should be an easy question for any SaaS provider to answer. Whether the data is being hosted by a cloud service provider, such as AWS, or by the vendor themselves, there should be a documented data security plan. As part of that plan, the software vendor should be able to demonstrate how data is protected through physical and logical separation within the system and the application of robust encryption to the data both at rest and in transit. Additionally, the vendor should have a well-documented information security management system (ISMS), which can be further evaluated by third parties for adherence to SOC 2 Type 2 and ISO 27001.
What is your uptime SLA?
SaaS providers should provide uptime guarantees in writing, typically within a Service Level Agreement (SLA). The majority of SaaS business software providers will offer uptime guarantees between 95% and 99%. For mission-critical solutions, such as RIM systems, expect guarantees at, or close to, 99%.
What happens to our data if we leave?
Because you are not storing your data locally, be sure to understand what will happen to your data if you choose to terminate your contract with a SaaS solution provider. You should be able to access your data after termination, download data prior to termination, or both. Ask if you will be charged for this.
Can I access and report on all of my data, all of the time?
It is important to know that you will be able to access all of your data at any point in time, especially during an audit or inspection. Can you create reports that reference any and all data fields in the system? Will older data be archived automatically at any point? Are there API’s available to allow other systems to access the data?
What are your fees based on?
SaaS companies can base their fees on a variety of factors, including data usage, number of users, and features used. Be sure to understand all of the factors that may affect your subscription fees now and in the future.
SaaS terms to know
- SLA: An SLA is a “Service Level Agreement,” which serves as the contract defining what the SaaS vendor is providing and what the customer expects to receive. Among other things, the SLA will define uptime guarantees, what counts as downtime, the procedures followed in the case of a data breach, and how termination of the contract is handled.
- Uptime: Uptime is the percentage of time during which the SaaS software is operational and available to subscribers. The specifics of how uptime is measured should be part of the SLA. Downtime is the converse of uptime.
- API: API, or Application Programming Interface, is a set of definitions and protocols provided by software applications to allow data sharing and integration between applications.
- Module: A part of the software platform that is dedicated to a specific function and outcome. SaaS pricing is often organized around the purchase of one or multiple modules.
- Feature: Specific functionality in the software that comes together to achieve an outcome.
Want to learn more about SaaS solutions for regulatory information management? Contact us to schedule a custom demonstration.

Global strategy for Unique Device Identifier (UDI) data
The International Medical Device Regulators Forum (IMDRF) developed a UDI framework for a globally harmonized system for the identification of medical devices. Adopted in principle by regulatory authorities in many countries, the implementation of UDI regulations and supporting databases is at varying stages of implementation across the globe.
UDI Components
Establishing a UDI strategy involves understanding requirements for both labeling and regulatory database reporting in each country in which your devices will be marketed.
UDI labeling
The UDI is typically presented as a barcode label on device packaging or the device itself (depending on specific requirements). The UDI consists of two major components:
- UDI-DI - This is the static portion of the UDI which identifies the manufacturer along with the specific device version. The UDI-DI (device identifier) is assigned by an approved organization, such as GS1, and contains a company prefix and the manufacturer's internal product code. The UDI-DI is the primary identifier to be used in looking up device attributes in country-specific databases and is assigned prior to placing a product on the market.
As GS1 is widely recognized as an issuing agency across global regulators and industry, the UDI-DI is often referred to in the GS1 nomenclature of Global Trade Item Number (GTIN). - UDI-PI - This is the dynamic portion of the UDI which is assigned by the manufacturer and identifies a manufacturer’s lot number, serial number, manufacturing date, expiration date, or other data as required. The UDI-PI actual values do not appear in country-specific UDI databases, but these databases often require information about the type of data that the UDI-PI represents on the device label.
UDI regulatory database requirements
Many countries have established, or are in the process of establishing, databases to store UDI data. In the United States, use of the Global Unique Device Identification Database (GUDID) is mandated for medical devices. In the EU, EUDAMED consists of multiple modules with one specifically established for UDI. The UDI module is currently available for voluntary use, with mandated compliance scaled in transitional periods through 2026.
Currently, the US GUDID database provides for machine-to-machine (M2M) transmission of data, allowing manufacturers to upload product UDI data directly into the database. The EU has established requirements for M2M transmission as well, but these requirements are not finalized. Most other countries do not have M2M capabilities at this time.
Universal UDI ®
While each country defines specific UDI data requirements, there is a core set of data that is consistent across many markets. At Rimsys, we refer to this data as the Universal UDI® data. Storing Universal UDI® data separately from any country-specific UDI data is an important data management strategy. This ensures that data is single-sourced and consistently applied across submissions to regulatory UDI databases and in other locations in the manufacturers’ quality management system where the data may be needed.
When storing UDI data locally, consider that the same information may be required in different formats in different country regulatory databases. Currently, Rimsys supports the specific data requirements of the US, EU, Saudi Arabia, China, South Korea, and Singapore. Additional countries, which are expected to have similar IMDRF style requirements, will be added as those databases are established by regulators and brought to the industry. Some examples of these countries are Australia, Switzerland, UK, Brazil, and India.
Note that outside of the US’s GUDID, UDI databases are in flux in most countries. This means that having a central RIM system to track known and well-established UDI data is increasingly important.
Machine to machine transmission of UDI data
Machine to machine (M2M) transmission is the process in which data is transmitted from a company’s internal database, typically a RIM or PIM/PLM system, to the regulatory UDI database. Currently, the GUDID database in the US is the only database for which machine to machine (M2M) transmission has been fully developed and is fully supported. Rimsys offers M2M data transmission for GUDID and is currently working to establish M2M transmission with EUDAMED.
Synchronizing UDI data
It is important to note that there are really no requirements for a medical device manufacturer to keep a quality record of the UDI data submitted to regulatory databases (the official data of record is the data that has been reported to and is retrievable from the regulatory database). This means that it is up to the manufacturer to declare the actual source of data for the quality system and to ensure that data is in sync where required.
One of the strategies that can be used when implementing a new RIM system, such as Rimsys, is to export data from GUDID, EUDAMED, and other regulatory UDI databases. That data then forms the basis for the UDI data that is input into the RIM system, ensuring consistency in the application of data across other countries’ UDI databases.
Maintaining and updating submitted UDI data
It is important to implement procedures to ensure data in a product’s UDI record is consistently applied throughout your internal systems as well as with the various regulatory databases. While a single data point should be stored in as few places as possible, everything should be done to minimize the chances that data will get out of sync.
Any product data changes must be evaluated for, among other things, the effect on existing UDI data submissions to regulators. The data changes must be evaluated to determine if the UDI-relevant data can be updated in impacted regulatory databases or if an entirely new UDI-DI and record must be reported. In some cases, such as a change to the product’s catalog number or contact phone number, an existing UDI record may simply need an update. In other cases, such as a change to the sterilization requirements, a new UDI-DI and a new record may be required.
EUDAMED considerations
The EUDAMED database and M2M requirements for UDI are still not finalized, but they are much more static than they were even a month or two ago. We believe that it is beneficial for medical device manufacturers to establish and organize the data needed to submit their products to EUDAMED as soon as possible.
Legacy devices are those medical devices and In Vitro Diagnostic (IVD) devices that are compliant to previous directives (MDD, AIMDD, IVDD) that are being placed on the EU market under the allowed transitional period. With the compulsory application of EUDAMED identified in the 2026 timeframe and the expiry of the transitional period in 2024, there was no need for manufacturers to register legacy devices in the EUDAMED system. Today, with the extension of the transitional period for the certification of devices under MDR and IVDR through 2027, legacy devices may now again be subject to submission of UDI data in EUDAMED.
There will be a 24-month transition period for manufacturers to apply UDI data to EUDAMED once all modules go live. However, if you have any type of action requiring interaction with the Vigilance module of EUDAMED, the required UDI information for those devices must be present in EUDAMED prior to that interaction. The Vigilance module is intended to manage all types of vigilance reports, including Manufacturer’s Incident Reports (MIR) and Field Safety Corrective Action (FSCA) reporting. This also includes and requires post market surveillance reporting submission to the Vigilance module such as Periodic Safety Update Reports (PSUR) and Post Market Surveillance Reports (PMSR).
Manufacturers may be surprised with a shortened transitional period for compliance to EUDAMED’s UDI module due to this requirement and should place priority on higher-risk devices due to the increased likelihood of an interaction with EUDAMED’s Vigilance Module.
For additional resources, watch a replay of our webinar, Why UDI is a regulatory concern, not just an operation process - or read our eBooks, The Ultimate Guide to EU MDR/IVDR UDI and The China NMPA UDI System.

Educational resources for medtech regulatory affairs professionals
Staying on top of changing regulations and expectations is challenging for MedTech regulatory professionals around the world. The following list is some of the educational resources that are most used by RA teams to stay current. With the exception of RAPS, we focused primarily on resources provided by regulatory agencies directly. Rimsys does not endorse or validate information on these sites.
Professional Organizations
Regulatory professional organizations provide a combination of free and paid training courses and certifications.
RAPS
The Regulatory Affairs Professionals Society (RAPS) is the first stop for most regulatory professionals looking for education and certification:
- Courses (open to non-members) - includes RAC exam prep, online courses, webinar replays, and training bundles
- Learning portal (RAPS members only)
- Connect RAPS (RAPS members only forum)
TOPRA
TOPRA is a professional membership organization for individuals working in healthcare regulatory affairs. TOPRA was founded in the United Kingdom and is active in Europe.
Regulatory Agencies
United States (FDA)
The FDA offers a variety of free educational resources, including live and on-demand webinars, along with written documentation:
- Training and Continuous Education home page
- Continuing education programs
- CDRH Learn
- Guidance Webinars
EU Medical Devices Sector
- Event list (including educational webinars)
- Publications (including step-by-step guides)
- EUDAMED information center
Canada
- e-Learning courses on how medical devices are regulated in Canada
Singapore
While these are not training modules, the following free “tools” are available from the Singapore Health Sciences Authority:
- Is it a medical device?
Answer a series of questions to determine if your device is considered a medical device in Singapore. - Risk classification tool
Answer a series of questions to determine the risk classification of your medical device. - Registration and licensing requirements
Answer a series of questions to determine the correct registration route. - Medical device grouping tool
Answer a series of questions to determine if you can group your medical devices together for registration.
Additional third-party resources
Some sites that we find particularly useful. Note that Rimsys has no business relationship with these sites.
Paid Resources
Notified Bodies and other large consulting firms can provide detailed training options, but these organizations are in the business of providing expert consulting and education, so these options are not free. Those listed here provide individual, self-service, training courses that are charged per-session:
If you have any additional resources that you think we should include here, please connect with us on LinkedIn or Twitter!

FDA predicate devices
Medical device manufacturers seeking to place a new device in the U.S. market through a 510(k) submission are required to identify a legally marketed device that is substantially equivalent to the new device – i.e.: the predicate device. Selecting the correct predicate device is extremely important in ensuring the success of your 510(k) submission. New devices without a predicate are automatically classified as Class III devices requiring a premarket authorization (PMA) submission (although those with a lower risk profile can apply for reclassification through a De Novo request).
Predicate device requirements
A predicate device is used in a 510(k) submission to demonstrate that the new device to be marketed is safe and effective. This is done through establishing substantial equivalence between the predicate device and the new device. The predicate device must be a legally marketed device approved through a 510(k) submission, to which equivalence can be demonstrated. In identifying a predicate device, preference should be given to devices which are currently marketed in the U.S. and which have received 510(k) clearance relatively recently.
Predicate devices may be:
- Postamendments devices – devices marketed after May 28, 1976. The majority of 510(k) submissions claim substantial equivalence to a postamendment device.
- Preamendments devices – devices which were legally marketed in the U.S. before May 28, 1976 and which have NOT been significantly modified and for which a regulation requiring a PMA application has not been published by the FDA.
- Either postamendment or preamendment devices which are no longer marketed in the U.S. In this case, the predicate device cannot be a device that is, or was, in violation of the FD&C act.
Substantial equivalence
A medical device is considered substantially equivalent to an identified predicate device if the devices share an intended use and meet either one of the following:
- Shared technological characteristics, OR
- Different technological characteristics that do not raise different questions of safety and effectiveness and the safety and effectiveness of the device is demonstrated by information submitted to the FDA.
It is also important that the predicate device selected does not use outdated or superseded technology, which means that newer devices tend to be used as predicate devices. Note that while substantial equivalence needs to be demonstrated, the devices do not need to be identical. However, if the FDA finds that substantial equivalence has not been demonstrated with the identified predicate device, the applicant may:
- Resubmit the 510(k) with new data
- Request a Class I or Class II designation through the De Novo classification process
- File a reclassification petition
- Submit a premarket approval application (PMA)
How to find a predicate device
The FDA provides a 510(k) database containing all devices cleared through the 510(k) process. This database is updated monthly and can be filtered by device class, product code, applicant name, and other information.
Before searching the 510(k) database, the device and product classifications should be determined. The best way to find the correct classification of a new device is to use the Product Classification database, which can be filtered by device name and review panel, along with submission type, product code, device class and more. Searching the 510(k) database with the correct 3-letter product code is typically the most effective way of finding potential predicate devices.
Using a reference device in a 510(k) submission
The identification of a “reference device,” in addition to a primary predicate device, can be used to “support scientific methodology or standard reference values.” A reference device cannot be used in lieu of a primary predicate device and the FDA will evaluate the appropriateness of the reference device.
Note that prior to a 2014 guidance, the FDA allowed for “split predicates,” or the use of one predicate device to demonstrate equivalence in intended use, and another to demonstrate equivalence in technological characteristics. The current guidance finds the use of split predicates "inconsistent with the 510(k) regulatory standard.”
The importance of selecting the right predicate device
Selecting the right predicate device is critical to ensuring that your device can be brought to market through the 510(k) pathway. Selecting the wrong device will result in delays to the regulatory approval process. If an applicable device with current technology cannot be identified, other pathways, including De Novo request and PMA submissions, should be considered. For additional information, read The Beginner's Guide to the FDA 510(k).

Medical device audits - preparation and responses
The word “audit” can strike panic in poorly prepared medtech companies. However, audits serve an important purpose in ensuring a compliant and effective quality system and production of safe and effective medical devices. And organizations can limit the stress and risk around audits through proper preparation.
The key to a positive audit is to ensure that your organization’s focus is on building and implementing quality processes and procedures that cover the entire product life cycle and are continuously evaluated and improved upon. Not only is it the right thing to do, but focusing too closely on simply passing an inspection or audit may leave gaps in your processes and present a false sense of compliance. This article covers audit basics, how to prepare for them, and what to do when you receive an audit finding.
What is an audit?
Per ISO 19011 an audit is a systematic documented and independent process for obtaining objective evidence and evaluating it objectively to determine the extent to which the audit criteria are fulfilled. Audits can be internally conducted, externally conducted by interested parties (i.e., customers/ suppliers), and externally conducted by government agencies and notified bodies to ensure that product design, manufacturing, safety, and documentation requirements are being met. Audits will verify compliance with regulatory and quality system/GxP (Good Manufacturing Practices, Good Distribution Practices, etc.) requirements. GxP standards are dictated by the US FDA, European Medicines Agency (EMA), the UK Medicines and Healthcare Products Regulatory Agency (MHRA), and other regulatory bodies which rely on country-specific regulations as well as standards developed by the International Organization for Standardization (ISO).
Audits are required regardless of device class, but audit requirements in the EU and US, along with most other markets, can be dependent on the device classification. For most medium to high-risk devices in the US and EU, the following audits take place:
- Audits by EU Notified Bodies: Audits by EU Notified Bodies focus on compliance with MDR 2017/745 or IVDR 2017/746. Notified Bodies are also responsible for certifying quality management systems (QSR) against the requirements of ISO 13485:2016. Periodic “surveillance audits” will also be performed, based on the classification of the medical device(s).
- FDA Inspections: The FDA will conduct inspections to ensure compliance with the quality system regulation, 21 CFR 820, and to confirm that a facility is capable of manufacturing the medical device. The FDA will conduct pre-approval inspections to verify data included in a market submission, along with periodic routine inspections, following the Quality System Inspection Technique (QSIT) as required by regulation (currently every two years for Class II and Class III USA-based device manufacturers and every five years for international device manufacturers).
- Unannounced and “for cause” inspections: Manufacturers in the US and EU, and many other markets, are subject to different types of inspections triggered by consumer complaints, reported non-conformities, or other issues. These “for cause” inspections may be scheduled or unannounced.
How to prepare for an inspection
Audit preparation is a continuous process that should be built into your quality system and regulatory processes. Some items to consider:
Internal Quality audits
The best way to prepare for an upcoming audit or inspection is to use the internal audit program to your benefit. The FDA QSR, FDA 21 CFR 820, calls for medical device manufacturers to perform regular internal audits of their systems and to provide evidence of these audits and their effectiveness. When possible, conduct internal audits as if you’re the regulatory body and take them seriously. Internal audits should find the issues before the regulators do. Issue nonconformances and address them in a timely manner.
Performing “mock” audits is another great way to prepare for external inspections/audits from the FDA, notified bodies, and other regulatory authorities. Mock audits are a rehearsal for your team to prepare them for the real thing. They can act as try-outs to determine who is equipped to handle being audited and those that are too nervous or offer too much information when asked a question, requiring additional training. Mock audits are typically separate from the internal audit program since they are conducted based on different objectives and for training purposes.
It’s common to contract an independent third party to perform mock audits. Consider conducting unannounced mock audits to get the truest picture of your company’s preparedness. In short, the tougher medical device manufacturers are on themselves while preparing for the audit, then the less stressful the actual audit will be.
Self-identify issues as they appear and do not wait for the internal audit. If an issue is identified during the audit preparation or mock audit, implement corrective and preventive actions (CAPA) to address the issue. This is vital to demonstrate that you are aware of an issue and have begun remediation or corrective actions if and when those issues are uncovered during the real inspection or audit.
Choose the right audit host
When you have an upcoming audit or inspection, you must choose the right company representative to host the auditor(s). The person you choose will represent your company, so be deliberate about selecting those who know the company, its quality management system, and its products well. It should also be someone you’re confident can perform well under pressure and remain mission-focused in managing the audit and not necessarily answering every question immediately. The audit host can significantly impact the audit for the better or worse, so be certain that you have the right person in place who will be able to represent the organization’s values and facilitate an efficient audit.
While the person or people working directly with the auditor(s) are often from your quality team, they will need to be supported by subject matter experts (SMEs) from other functions for the duration of the audit – this will include the regulatory, engineering, operations, and marketing teams – who can answer specific questions and gather requested documents. These SMEs must be pre-identified along with alternates as part of the audit preparation. They should be comfortable facing an auditor and answering the auditor’s questions.
Gather all the necessary documents
As part of the audit process, the auditor(s) will expect access to information that they need to determine your organization’s compliance with all quality system and regulatory requirements. Based on the requirements, audit guidance, and previous audits, commonly requested documents should be known. This documentation should be pre-identified, compliant, and available before the start of an audit. This can be in the form of hard copies or electronically through files or links. The goal is to have documents readily available to avoid audit delays.
"If it takes too long to get documents to the auditor when they ask for them, you’re not making a good overall impression that everything is under control, making things more difficult for the auditor(s). Auditors have schedules to meet and follow certain audit trails. The last thing you want is your auditor getting agitated because they are spending a lot of time waiting for information." - Bruce McKean, Rimsys Director of Regulatory Affairs
It is critical that all regulatory information related to your products is readily available during an audit, such as registration status, certificates, regulatory impact assessments, and essential principles, along with submission content and post-market data. A central RIM system that stores all regulatory data and links to (or references) the current versions of records from other systems, such as PLM, eQMS, and ERP systems, can smooth the audit process significantly.
During an audit
As an organization, you will want to manage as much of the audit process as possible. Your audit host will greet the auditor(s) and give them a brief overview or presentation of your company, and most likely conduct a facility tour. After this, while the auditor(s) will direct the process, the more your host can assist and guide them, the better.
In the case of unannounced inspections/audits, there must be a procedure in place that defines how to receive and handle these types of audits. This will include who is the primary contact during such an inspection (often a Quality Management team member or representative), as well as Executive Management, and alternates when those people are not available.
Ideally, you should have more than one company representative with the auditor(s) during the audit and auditors should not be left alone at any point. Most companies have a team in the “front room” with the auditor(s) led by the audit host. The main job of this team is to transcribe every question, answer, and activity that occurs during the audit. The “front room” team will communicate with other team members in the “back room” in real-time (often via instant messaging), relaying to them any open questions, requested documents, or queuing up SMEs the auditor(s) need to speak with.
Best practices for sharing information with auditors
During an audit, employees should be cooperative and helpful, but should only share information that is specifically requested by the auditor. If information is requested that seems outside the scope of the audit, such as corporate strategic or financial documents, employees should notify the appropriate executive before providing such information.
Auditor(s) should be given access to requested information through photocopies or limited computer system access. Original documents can be presented if requested, but should never be kept by the auditor(s). All information provided should be prepared, verified, and recorded in the “back room” and then passed through to the audit host so that it can be controlled. The “back room” should mark the copies “Confidential” or “Proprietary,” as appropriate. They should also make an extra copy for the audit file, so the exact documentation given to the auditor(s) is known for future reference.
Addressing missing or incorrect information
Ideally, any potential issues with the existing quality system and related procedures are identified before an audit and corrective actions are identified and put in place. Even in cases where an issue has not been fully resolved, being able to point to awareness and appropriate actions is important.
Some findings may be able to be corrected during the audit. These findings are typically isolated issues (one-offs) that do not pose significant risks. For instance, a missing revision number, missing signature, or outdated reference. If corrected during the audit, it may negate a finding, but the auditor may want to understand why the issue occurred and what actions you have or will be, taking to ensure that it does not recur.
In cases where you are unable to produce the information requested by an auditor, or when there are questions about the validity or accuracy of the information, your internal team should acknowledge the issue but should not immediately speculate on the cause or the effect of the missing or inaccurate information. A discussion of appropriate actions under the existing quality system may be appropriate.
What to do in case of a finding
Be prepared to receive findings from any inspection. Ideally, the auditors should be working to ensure that you are compliant with regulatory requirements and that your records accurately state what you do. However, “By the nature of the beast,” says Bruce McKean, “they’re there to find instances of noncompliance.” This means that auditors will be focused on documentation that can prove or disprove adherence to your stated procedures and policies.
All findings should be disclosed before the audit closing meeting. There should be no surprises. Ensure that the findings are understood by both parties. If they are not clear, perhaps the auditor misunderstood or did not see specific objective evidence and you should discuss or review the issue with the auditor as this may negate a finding. Be sure to debrief upper management before the closing meeting. At the audit closing meeting, there should be no debate over findings. Any finding, whether major or minor, should be addressed diligently.
Audit findings or observations will result in the regulatory body in charge of the audit issuing a document that lists those findings. In most cases, you will have limited time to respond with a satisfactory plan for correcting and preventing the recurrence of the identified issues.
In the case of the FDA, multiple enforcement actions are available to the agency, ranging from warning letters to criminal prosecution. Note that many regulatory agencies will not respond further to your actions if they agree with the actions you prescribe for addressing audit observations. However, additional actions may be triggered if your response is not found to be satisfactory.
Rimsys is a holistic regulatory information management system designed for and by regulatory affairs professionals. Rimsys makes it easier to create and track submissions, keep up with product registrations and certificates, and even share pertinent data across ERP, PLM, and eQMS software platforms to ensure data integrity. Learn more about how Rimsys can help you face audits with the confidence that you have all of your regulatory ducks in a row.

Australian Essential Principles
The Therapeutic Goods Administration (TGA), under the Australian Department of Health and Aged Care, is responsible for evaluating, assessing, and monitoring products that are defined as therapeutic goods. They regulate medicines, medical devices, and biologicals to help Australians stay healthy and safe.
Manufacturers are responsible for generating, collating, assessing, and maintaining scientific and engineering evidence that shows that their devices comply with the Essential Principles. The evidence must be relevant to the device's intended purpose and must be objective, sufficient, and robust. Manufacturers manage this by having a solid, quality management system (QMS).
An ‘Essential Principle’ is fulfilled during the design and manufacturing of medical devices and IVD medical devices, to ensure that they are safe and perform as intended. A global adoption of a common set of fundamental ‘essential’ design and manufacturing requirements for medical devices provides significant benefits to, among others, manufacturers, users, patients/consumers, and to regulatory authorities. From a high-level perspective, three basic points make up ‘Essential Principles’:
- A device must be designed to be safe and perform effectively throughout its lifecycle.
- Device manufacturers must maintain all design characteristics.
- A device must be used in a way that is consistent with how it was designed.
Many countries use the term ‘Essential Principles’ (EP's) in regulations and guidance documents. ‘Essential Requirements’ is the terminology used in the EU MDD 93/42/EEC and AIMD 90/385/EEC. With the release of the MDR/IVDR, they are now referred to as GSPR's (general safety and performance requirements). Regardless of the terms used, Essential Principles are of similar nature and overlap many of the Essential Requirements in the new GSPRs.
Demonstrating Compliance
It is the manufacturer’s responsibility to demonstrate that their medical device is compliant. The TGA’s regulatory process does not necessarily dictate “how” a manufacturer must demonstrate compliance with the Essential Principles. However, there is a range of data points that are suggested to be used as objective evidence to show that your device complies with the Essential Principles. Listed below are some examples of the data you would want to track and list in your Essential Principles documentation, commonly referred to as The Essential Principles Checklist or GSPR’s.
Details of design and construction:
- a general description of the medical device and its intended purpose
- specifications, protocols, procedures, and details of design and development methods, and technologies used for manufacturing, packaging, storage, handling and distribution
- procedures for measuring and monitoring the safety, performance, and quality of your device
- procedures for servicing (if appropriate)
- procedures for assuring your medical device is sterile (if appropriate)
Risk management reports:
- risk analysis
- risk evaluation
- identification of residual risks
- controls of known and foreseeable risks
Demonstrate compliance with relevant, generally acknowledged state-of-the-art and best-practices:
- technical standards, guidelines, or other validated methods
- codes of practice
- monographs
Characterization studies:
- Verification and validation activities, including protocols, testing and analysis.
- Records of qualitative or quantitative information obtained through observations, measurements, and tests.
Clinical evidence:
- literature reviews that include information about the hazards and associated risks from the use and potential misuse of the device.
- information about the performance of the devices you are manufacturing, including a description of the techniques used to examine whether devices of that kind achieve their intended purpose or not.
- Collation and analysis of post-market data including complaints, adverse-event reports, vigilance reports, registry data and recalls/field corrections/advisory notices.
Additional information:
- Copies of labels, packaging, patient information, and instructions for use.
- Critical evaluation written report, by an expert in the relevant field, of data (including outcomes from literature reviews) about your device.
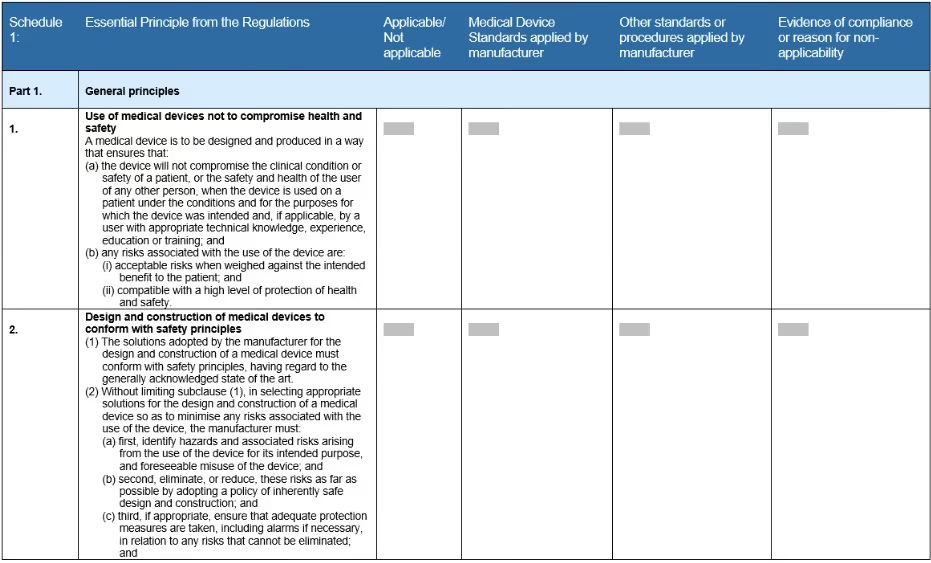
Essential Principles checklist
The checklist is a form template that the TGA created for medical device manufacturers. It lists all the necessary requirements that must be met, as part of the technical file, to demonstrate regulatory compliance. It’s structured in a table format with each general principle clearly stated with instructions on how to complete the form (Fig 1).
The TGA follows the guidelines of the International Medical Device Regulators Forum (IMDRF). They were one of the founding members to take part in the IMDRF that was established in 2011, building off the groundwork of the Global Harmonization Task Force (GHTF). Today there are 11 countries that participate in accelerating international medical device regulatory harmonization. This group of regulators provide input to policies, offer guidance on strategies, create clear directions - all in an effort to help build a strong foundation for the safety of the medical device industry.
For additional information on Australian medical device regulations and links to resources, see our Australia Regulatory Market Profile. For information on the use of essential principles in the EU, see The ultimate guide to the EU MDR and IVDR general safety and performance requirements (GSPR).
