
FDA device registration overview
Registering a new medical device with the FDA can be a huge undertaking, and understanding the process and all of the requirements as early as possible is important. This article provides a high-level overview of the steps required before marketing and selling a medical device in the United States. We’ve done our best to include relevant links to both FDA documentation and educational materials wherever possible!
FDA medical device registration steps
Classify your medical device
Classifying your medical device should be one of the first steps in any FDA submission. The FDA classification system is a “predicate-based” system in which devices are classified based on similar devices that are already on the market in the U.S.
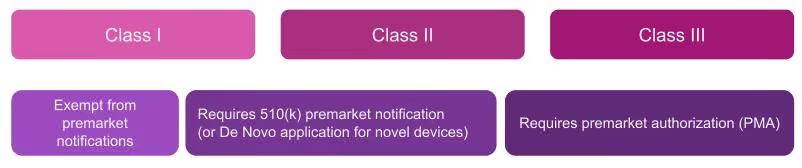
You may already have an idea as to which of the three device classes your product falls under, but you still need to determine the specific device category described within 21 CFR Parts 862-892. The FDA provides a good overview and listing of device categories that is searchable. This will allow you to determine which specific section of the regulation pertains to your device, which will then define the classification and relevant premarket requirements. While the majority of Class I devices require no premarket notification, the majority of Class II devices require 510(k) premarket notification, and the majority of Class III devices require a premarket authorization submission, however,this is not always the case.
Medical device manufacturers can request information and guidance from the FDA regarding the classification of a device through a 513(g) request. For the classification of accessories to your device, a pre-submission may be more appropriate (discussed below)
Collaborate with the FDA prior to your submission
The FDA encourages pre-submission collaboration meetings and communication as early in the product development process as possible. It is in the best interest of organizations seeking approval of a medical device to have an open dialogue with the FDA, enabling the FDA to advise before and during the submission process, provide direction on Investigational Device Exemption (IDE) applications, and identify any potential concerns that may affect approval or clearance of the device. This is especially important for devices with novel technology.
There are a number of pre-submission activities defined in the FDA’s “Q-Submission” program (these were previously referred to as “pre-ide” meetings). Q-subs provide an organization with the opportunity to obtain feedback from the FDA before a premarket submission is made. The most common Q-subs are:
Pre-submission (pre-sub) requests provide an opportunity for an organization to obtain feedback from the FDA before completing a premarket submission. Pre-sub requests are made in writing to the agency and can involve a meeting if requested by the submitter. The submitter should have specific questions prepared regarding their submission and/or product development prepared for the FDA to review during this meeting.
Informal Meetings are requests to share information with the FDA with no expectation of feedback. This may be helpful if your team has a variety of submissions planned, or if your company would like to explain the technology of your device.
Early collaboration determination meetings are requests by a PMA applicant for the FDA’s determination of the type of valid scientific evidence required to demonstrate that the device in question is effective for its intended use.
Early collaboration agreement meetings are used to reach an agreement between the FDA and the submitter on key parameters of the investigational plan.
Results of early collaboration determination and agreement meetings are binding on the agency. For additional information, see “Early Collaboration Meetings Under the FDA Modernization Act: Final Guidance for Industry and for CDRH Staff”
Prepare the appropriate premarket submission for your medical device
Remember that most Class I devices, and some Class II devices require no premarket submission (though they are required to be listed with the FDA).
510(k) Premarket Notification is used for Class II and Class III devices with a medium risk profile for which there is a predicate, substantially equivalent, device on the market that requires a 510(k) submission.
The 510(k) submission is used to demonstrate that the predicate device is substantially equivalent to the new device and, if successful, results in an FDA “clearance” for the new device. You can read more in our FDA 510(K) beginner’s guide.
Premarket Approval (PMA) is used for Class III devices for which the identified predicate device requires a PMA. These are devices which are high risk; defined as a device that supports or sustains human life, is of substantial importance to preventing impairment in human health, or presents a potential and unreasonable risk of illness or injury. Novel devices which have no substantial equivalent on the market also require a PMA by default.
A PMA is intended to prove that a new device is safe and effective for the end user, and is much more detailed and in-depth than a 510(k). Device manufacturers are typically required to present human clinical trial data, in addition to laboratory testing data. A successful PMA results in an FDA “approved” device.
The De Novo classification process can be used for novel devices for which there is no substantial equivalent on the market, but which have the lower risk profile of a Class I or Class II device. A successful De Novo request is “granted” by the FDA and results in the classification of the device as Class I or Class II. You can read more in our De Novo classification process: a beginner’s guide.
Work with FDA staff during the review process
The more complex your submission to the FDA, the more opportunities you will have to interact with the agency during the review process. Take advantage of these opportunities and be sure to respond to any requests for additional information within the specified time frame. The 510(k) submission process and the PMA submission process both have defined procedures for requesting and submitting additional information during the review process. PMA submissions for devices with new technology may also require interaction with an expert review panel.
If you need additional clarification from the FDA on your 510(k) or PMA submission, the following options are available: through the Q-submission process:
Submission Issue Requests (SIR) are Q-submission requests for feedback and clarification during a pre-marketing submission including 510(k), De Novo and PMA submissions. These are often held after a submitter receives letters from the FDA asking for additional information or deficiency letters.
PMA day 100 meetings are Q-submission requests held within 100 days of a PMA submission and are used to discuss any deficiencies in the application, and to begin a conversation on the status of the application. FDA guidance on PMA day 100 meetings can be found here.
Complete a quality system audit
Most Class II and III devices, and some Class I devices will require a premarket quality system inspection. During most of the Covid pandemic, inspections were being conducted remotely, but the FDA resumed domestic onsite inspections in February 2022.
A compliant quality system demonstrates that your facilities are capable of manufacturing the device as designed to meet its intended purpose, and the FDA will evaluate both design controls and manufacturing controls.
Current quality system requirements are defined in 21 CFR part 820 (quality system regulation or “QSR”), however the FDA is moving to harmonize their requirements with the generally accepted global standards of ISO 13485. In addition, the Medical Device Single Audit Program (MDSAP) can be used as an alternative allowing a single audit that is recognized by regulatory authorities in multiple countries, including the FDA.
Whichever path your inspection takes, it is important to put a strong quality system in place as early as possible.
List your medical device on your establishment registration
Any organization involved in the production or distribution of a medical device intended for use in the United States is required to register annually with the FDA. Establishment registration is defined in 21 CFR Part 807. There is an annual registration fee, which is $5,672 for 2022.
Most establishments that are required to register with the FDA must also list the devices and the activities performed on those devices at the establishment. Registration and listing information must be submitted to the FDA within 30 days of a device being put into commercial distribution. You cannot list your device until it has been cleared or approved through a premarket submission process, if required for your device.
The FDA provides detailed information on the device registration and listing process.
Post-market compliance
We will cover post-market surveillance and compliance in a future post, but here are a few things to keep in mind:
- If your device was approved via a PMA, expect a post-market inspection 8-12 months after approval.
- Changes to a cleared or approved product may trigger additional reporting and submissions. The significance of the change will dictate the type of reporting required for both 510(k) cleared devices and PMA approved devices.
- Your quality system should include a CAPA (corrective and preventive action) tracking system to record and address any issues that arise after the device is on the market.
For additional information on FDA submission processes, see our ebooks which cover the 510(k), and De Novo processes.


GET IN TOUCH



.avif)
