


Featured
Rimsys Announces Rimsys AI to Eliminate Repetitive Tasks and Enhance Decision-Making for MedTech Regulatory Teams
Rimsys, the leading Regulatory Information Management (RIM) platform for the MedTech industry, today announced the launch of Rimsys AI, a suite of embedded artificial intelligence (AI) agents.

The ultimate guide to the EU MDR and IVDR general safety and performance requirements (GSPR)
This article is an excerpt from The ultimate guide to the EU MDR and IVDR general safety and performance requirements (GSPR) ebook.
Table of contents
- Overview
- Terminology
- EU MDR/IVDR Annex I
- EU MDR/IVDR Annex II
- Proactive Monitoring & Maintenance
- Comparison Table: EU MDR/IVDR Annex I GSPRs vs EU MDD/IVDD Annex I Essential Principles
With the initial rollout of the European Medical Device Regulation (MDR) complete, medical device companies are shifting focus to the sister In Vitro Diagnostic Regulation (IVDR) which has rolling effective dates starting in May 2022. Like the MDR, the IVDR also includes new General Safety and Performance Requirements (GSPR). The expanded 2nd edition of this ebook includes a detailed summary of the IVDR GSPR regulations in addition to those of the MDR. It provides you with practical guidance on how to meet the GSPR requirements for all types of medical technology products. This ebook, however, should not take the place of reviewing the actual regulations and consulting regulatory experts when needed
Timeline
The EU MDR submission became mandatory from the previous MDD directive on May 26, 2021, and the EU IVDR effective date is quickly approaching. In fact, all submissions for new devices under the new EU IVDR must be implemented no later than May 25, 2022. Below is a high-level overview of key dates for both regulations.
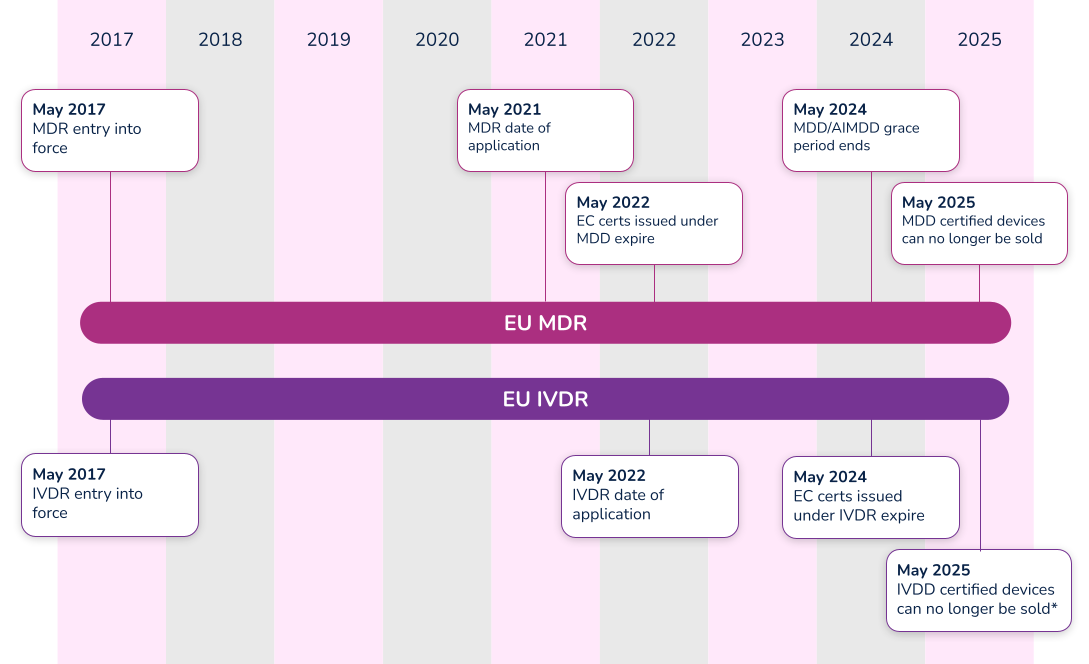
*Note that the timeline for compliance was extended in 2021. Class D (high-risk) devices have until 2025 to comply with IVDR, while Class C devices have until 2026. Class B and Class A sterile devices have until 2027 to comply with IVDR.
What’s the difference between Essential Requirements, General Safety and Performance Requirements (GSPR), and Essential Principles. In order to have a meaningful dialogue, let’s first discuss the three (3) main terms used in the industry.
#1 Essential requirements
The ‘Essential Requirements’ is the backbone for establishing conformity with the Medical Device Directive (MDD 93/42/EEC) and the Active Implantable Medical Device Directive (AIMDD 90/385/EEC). Detailed within Annex I of the MDD and AIMDD, the ‘Essential Requirements’ laid out the requirements that devices must meet in order to state compliance to the directives. With the implementation of the new EU Medical Device Regulation (MDR 2017/745), the ‘Essential Requirements’ will become superseded by the new EU MDR General Safety and Performance Requirements (GSPRs).
#2 Essential principles
The IMDRF laid out Essential Principles requirements in a document entitled Essential Principles of Safety and Performance of Medical Devices and IVD Medical Devices. From a high-level perspective, three basic tenets make up these ‘Essential Principles’:
- A device must be designed to be safe and perform effectively throughout its lifecycle.
- Device manufacturers must maintain all design characteristics.
- Devices must be used in a way that is consistent with how it was designed.
Many countries use the term ‘Essential Principles’ when compiling the documentation required to determine compliance to the law. For instance, the Australian Therapeutic Goods Administration (TGA) uses the term ‘Essential Principles Checklist’. Regardless of the term used, Essential Principles are of similar nature and overlap many of the Essential Requirements and new GSPRs.
#3 General safety and performance requirements (GSPR)
As of May 26, 2021, medical device manufacturers must start to comply with Annex I – General Safety and Performance Requirements (GSPRs) of the new EU Medical Device Regulation (MDR 2017/745). GSPRs are specific to the European MDR and IVDR. If you hear any other term (i.e. Essential Principles), it most likely means it is not referencing the European market.
Annex I of the EU MDR and IVDR details the specific requirements of the General Safety and Performance Requirements (GSPRs). The GSPRs are broken down into three (3) chapters in Annex I, MDR 2017/745 and IVDR 2017/746:
- Chapter 1 - General requirements
- Chapter 2 - Requirements regarding design and manufacture
- Chapter 3 - Requirements regarding the information supplied with the device
Chapter 1 - General requirements
Both the EU MDR and the EU IVDR outline General Safety and Performance Requirements (GSPRs) in great detail for medical device designers and manufacturers. The general requirements for each are almost identical and consist of the following:
- Devices must perform in a way that aligns with the intended design.
- They must not compromise the health or safety of a patient, user, or any other person associated with the device.
- Risks must be reduced as much as possible, but not so much that they negatively affect the risk-benefit ratio.
- Device manufacturers must implement and maintain a thorough, well-documented, and evaluative risk management system that continues to be updated throughout the life cycle of a device.
- Manufacturers and designers must include any necessary measures for protecting users in cases where risks cannot be completely eliminated.
- Manufacturers must provide users with information about any potential risks that remain. This information must be clear, easy to understand, and considerate of the users’ technical knowledge level, use environment, and any applicable medical conditions.
- Devices must withstand the stresses of normal use for the duration of their lifecycle. Devices must be designed, manufactured, and packaged in a way that protects them from damage during transport and storage.
- When it comes to risks and negative side effects that are known and foreseeable, designers and manufacturers must make every effort to minimize negative outcomes. They must also ensure that potential risks are acceptable when compared to the potential benefits of a device to its users.
Chapter 2 - Requirements regarding design and manufacture
The GSPRs also provide key details regarding specific information about the performance, design and manufacture of medical devices. As it relates to design inputs, the MDR and IVDR GSPRs provide highly detailed requirements relating to a device’s technical information. Further detail can be found in the comparison tables in Appendix A and Appendix B, where we have compared MDR to MDD and IVDR to IVDD.
Chapter 3 - Requirements regarding the information supplied with the device
The final key area of governance within the GSPRs relates to specific information a manufacturer must supply with a device. The general requirements for this information states that, “Each device shall be accompanied by the information needed to identify the device and its manufacturer, and by any safety and performance information relevant to the user, or any other person, as appropriate.” The requirements provide further detail as far as location - specific information that must be provided on the following:
- The device label includes its UDI.
- The user instructions.
- The packaging of a device that is intended to maintain its sterile condition.
Medical devices are subject to significant regulations and a full understanding of EU MDR and/or IVDR labeling as defined in Annex 1 Chapter 3.
In addition to the specific requirements identified within Annex I of the EU MDR and IVDR, Annex II, Technical Documentation, identifies additional requirements. Specifically, in both EU MDR and IVDR’s Section 4 – General Safety and Performance Requirements it states:
“the documentation shall contain information for the demonstration of conformity with the general safety and performance requirements set out in Annex I that are applicable to the device taking into account its intended purpose, and shall include a justification, validation and verification of the solutions adopted to meet those requirements. The demonstration of conformity shall include:
(a) the general safety and performance requirements that apply to the device and an explanation as to why others do not apply;
(b) the method or methods used to demonstrate conformity with each applicable general safety and performance requirement;
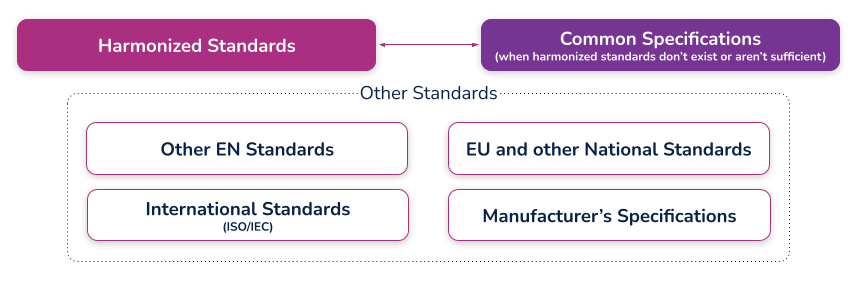
(c) the harmonised standards, CS or other solutions applied; and
(d) the precise identity of the controlled documents offering evidence of conformity with each harmonised standard, CS or other method applied to demonstrate conformity with the general safety and performance requirements. The information referred to under this point shall incorporate a cross reference to the location of such evidence within the full technical documentation and, if applicable, the summary technical documentation.”
Let’s break this down into each part.
Requirement
(a) the general safety and performance requirements that apply to the device and an explanation as to why others do not apply;
What needs to be documented for the requirements that apply or the requirements that do not apply?
Each and every section of the EU MDR GSPR or EU IVDR should be assessed in its own right as it pertains to your medical device. When a requirement applies, a simple statement may be made that this requirement applies to the device. In practice this is often achieved using a checklist or table, with a column for applicability and a Yes/No answer against each requirement. When a requirement applies, you can move on to the other parts of demonstrating conformity regarding methods used and standards applied.
When a requirement is not applicable, a statement must be made to that effect, i.e. a ‘No’ in the applicability column. Additionally, it must be fully and properly justified. Such a justification may be something like ‘The device is not powered and is therefore not an active device. This requirement does not apply.' The justification should clearly state why the requirement has been deemed not to apply so that your notified body can understand your reasoning
Requirement
(b) the method or methods used to demonstrate conformity with each applicable general safety and performance requirement;
What is meant by “method or methods used”?
This relates to the way you complied with that GSPR requirement, historically it would be listed as a standard or other documentation reference that you have applied to demonstrate compliance, however, the question of ‘method or methods used’ is new to the MDR and it is expected that a verbal description be provided such as:
i. Risk analysis weighed against clinical evaluation benefit
ii. Performance intended demonstrated by design requirements, verification and validation
Requirement
(c) the harmonized standards, common standards (CS) or other solutions applied;
What are harmonized standards, common specifications (CS), and “other solutions”?
Harmonized standards
These are standards that have been specifically developed and assessed for compliance to a regulation or directive. They are published in the Official Journal of the European Union (sometimes just referred to as ‘the OJ’) and if you comply with these standards then there is a ‘presumption of conformity’ with that directive or regulation to which they have been harmonized. These harmonized standards can only be created by a recognized European Standard Organization (such as CEN or CENELEC). When a standard is harmonized, an annex is added that describes how the standard conforms to the directive or regulation. When using harmonized standards, you should make sure that you understand how the standard conforms so that you do not claim compliance when the standard either does not meet that requirement or only partially meets that requirement.
If a standard does not meet a certain requirement of the directive or regulation, or indeed only partially meets it, then you must employ additional mechanisms for compliance. If a harmonized standard meets part of a directive or regulation, then by complying with that standard you also fully meet the corresponding requirement(s) The list of harmonized standards continues to grow - refer to the “Healthcare Engineering” section of the European Commission’s Harmonized Standards page for current information. In this case, using an MDD harmonized standard and documenting a justification for doing so (i.e. how you believe the standard demonstrates compliance with the GSPRs), should provide sufficient evidence
Common specifications
Common Specifications (CS) are a new concept in the MDR. They allow the European Union to add additional requirements that must be met in order to claim compliance where harmonized standards do not exist or where relevant standards are considered insufficient. The definition of a Common Specification is:
‘A set of technical and/or clinical requirements, other than a standard, that provides a means of complying with the legal obligations applicable to a device, process or system.’
Requirement
(d) the precise identity of the controlled documents offering evidence of conformity with each harmonized standard, CS or other method applied to demonstrate conformity with the general safety and performance requirements. The information referred to under this point shall incorporate a cross- reference to the location of such evidence within the full technical documentation and, if applicable, the summary technical documentation;
What is the expectation for incorporating a "cross-reference to the location of such evidence within the full technical documentation"?
This means that someone looking at the document should be able to identify exactly where in the technical documentation that the compliance evidence can be found. For example, this may refer to test reports and their exact location, or it could even reference locations within a large document, depending on the GSPR and your particular documentation. (i.e. if you have included usability risks as part of a larger risk assessment, you may need to say ‘See Technical File XXX, Section XX, Doc RMF001 rev 3 lines 65-78’). In other cases it could just mean the whole document reference, i.e. Have you done risk management? – then yes, it is RMF001 rev 3. What the specific reference actually is depends on how you have managed your technical documentation and how defined it is (i.e. separate reports or one big one). There should be no ambiguity as to where the document is located
An example of a completed GSPR checklist could look something like this (applicable and nonapplicable examples are shown):
Specification developers and manufacturers must continually maintain their technical documentation to stay compliant. Part of this process is to ensure that they take into account the "generally acknowledged state of the art".
Proactive monitoring
'State of the art'
There is no formal definition of ‘state of the art’ within the EU MDR or IVDR, although it is mentioned many times. ‘State of the art’ is an ongoing debate; however, it generally means that it embodies what is currently and generally accepted as good practice in the medtech industry. The ‘state of the art’ does not necessarily imply the most technologically advanced solution.
One consensus on state of the art is being up to date and compliant with the current and in effect standards that are applicable to your device. This means that if a standard is updated that your medical device is compliant with, you must evaluate that update to ensure that it would meet the EU MDR or EU IVDR ‘state of the art’ requirement. This is not a new requirement from the EU MDD but it is spelled out more clearly in the EU MDR.
The specification developer or manufacturer is ultimately responsible for determining if the updated standard applies or does not apply to their device(s). Either way, the justification should be documented within a gap analysis.
Monitoring for changes
Of course, 'state of the art' only applies if you actually know if something changed. This is why you need to develop a process for monitoring the standards that compliance is claimed. Every single standard that is associated with your technical documentation must be actively monitored, reviewed, and reported on.
If you have a product on the market and need a better way to monitor and maintain your General Safety and Performance Requirements (GSPR) or Essential Principles, Rimsys can help. Rimsys digitizes and automates GSPR and Essential Requirements so you can dynamically update and proactively monitor changing standards and evidence files.
When a standard or evidence file changes, you will automatically be notified and can update one GSPR or all of your GSPRs as applicable with a single click of a button. If additional information is needed, such as testing, it’s also invaluable to ensure that all devices are identified. What used to take weeks of manual, error-prone administrative tasks is now done in seconds within a fully validated, secure, maintenance-free, cloud-based solution
Maintenance
Maintaining and updating your technical documentation is generally the hardest part of staying compliant. Robust processes must be established to ensure nothing slips through the cracks and show up as nonconformances during regulatory audits.
Gap analysis
In addition to meeting the ‘state of the art’ requirements and the continuous proactive monitoring of standards, once a change has been detected that affects the technical documentation, a proper and thorough gap analysis must be completed.
The gap analysis between the old versions and the new versions, or an evaluation of a brand new standard, must occur and be properly documented. The gap analysis should detail what is applicable and what is not applicable, with your supporting justification.
If something within the new or revised standard was applicable to your device, additional engineering testing, documentation, justification, and, in some instances design changes, may be needed to ensure compliance
GSPR updates
Once the gap analysis has been properly documented, specification developers and manufacturers must update their GSPRs.
These updates include finding the withdrawn or superseded standard or evidence file throughout each row within your GSPR table, for every single device on the market on which this change is applicable. This could be one table or dozens of tables depending on the complexity of the products and your product mix.
Without a holistic RIM system to help you, this is an error-prone process as is it tedious, administrative, and extremely easy to miss an inappropriate referenced standard or evidence file.
Extreme diligence on the regulatory or engineering team must occur to ensure these critical updates to the GSPRs are not missed and a gap analysis must be properly referenced throughout. Any justification for including or excluding a new standard or evidence file will be scrutinized by regulatory auditors, and without proper maintenance, may lead to additional review time.
To continue reading this eBook including Comparison Table of the EU MDR Annex I GSPR vs. the EU MDD Annex I Essential Requirements, please register to download the full version.

The beginner's guide to the FDA PMA submission process
This article is an excerpt from The beginner's guide to the FDA PMA submission process ebook.
Table of Contents
- Introduction
- PMA basics
- FDA interactions
- Contents of a traditional PMA submission
- PMA supplements and amendments
- PMA Quality Management System (QMS)
- Review process and timeline
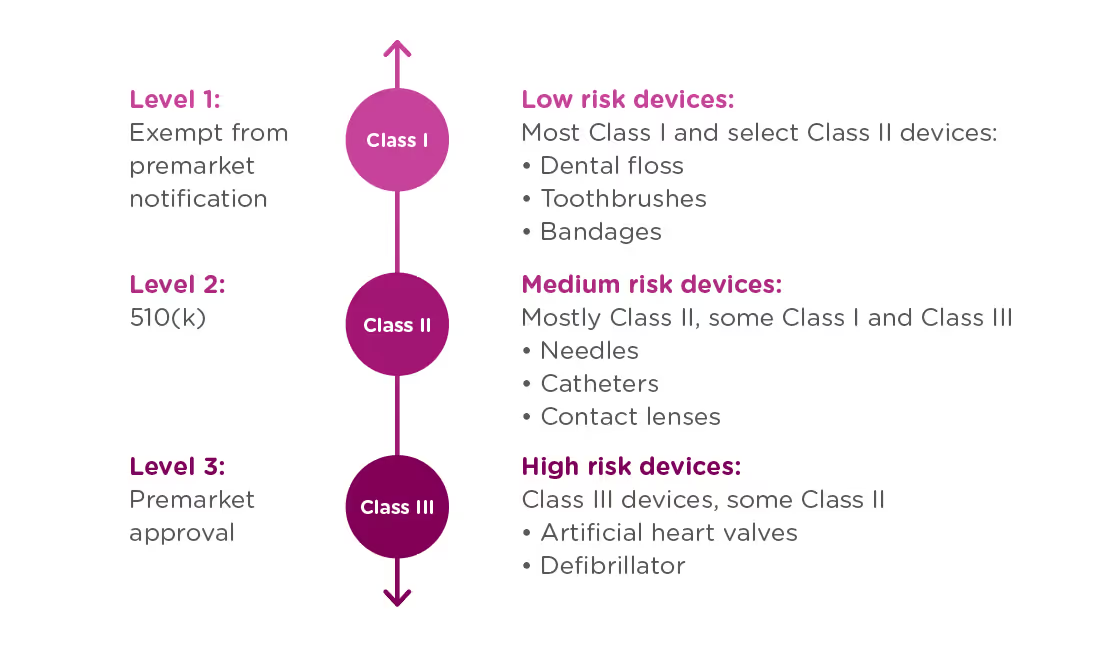
If your organization is planning to market a new medical device in the United States, you first need to determine which regulatory class the device falls under. The vast majority of medical devices regulated by the FDA are either Class I or Class II medical devices, requiring a 510(k) premarket notification or a simple registration if exempt from 510(k) requirements. However, if your device sustains or supports life, is implanted, or presents a “potential unreasonable risk of illness or injury,” your device is likely a Class III device which will require Premarket Approval (PMA) from the FDA before it can be marketed in the United States. Novel devices, for which there are no existing substantially equivalent devices, are automatically classified as Class III as well. Novel devices with a lower risk profile, however, may qualify for the De Novo process instead of the PMA. Just 10% of devices regulated by the FDA are Class III devices.
This ebook provides an overview of the PMA process and its requirements, but it is not designed to be the only resource used in compiling a PMA submission. The FDA provides significant documentation on this process, starting with the regulation governing premarket approval that is located in Title 21 Code of Federal Regulations (CFR) Part 814.
FDA: Background and device oversight
Before we explain what a PMA is, let’s first talk generally about the Food and Drug Administration (FDA) and device oversight. The FDA is the U.S. governmental agency responsible for overseeing medical devices, drugs, food, and tobacco products. When it comes to medical devices, the FDA’s mission is to “protect the public health by ensuring the safety, efficacy, and security of...medical devices.” At the same time, the FDA also has an interest in “advancing public health by helping to speed innovations.” In other words, the FDA’s goal is to make sure devices are safe and effective for public use, while also ensuring that devices have a quick and efficient path to market.
In order to achieve this balance of safety and efficiency, the FDA has three different levels of oversight depending on the risk level of the device: (1) exempt from premarket notification, (2) Premarket Notification, also known as 510(k), and (3) Premarket Approval (PMA).
When is a PMA required?
The PMA process is the most stringent regulatory process for medical device approval under the FDA and applies to almost all Class III devices. To determine whether your device requires a PMA, you must first Classify your device by searching the Product Classification Database. The database will provide you with similar devices; their name, classification, and link to the Code of Federal Regulations (CFR) if applicable.
- If a substantial equivalent is found in the Product Classification Database with a submission type of 510(k), you should submit a 510(k), not a PMA.
- If the product classification database identifies your device as Class III and/or requiring a PMA - you should submit a PMA.
- If your device involves a new concept and does not have a classification regulation in the CFR, the database will list only the device type name and product code. In this case, the three-letter product code can be used to search the PMA database and the 510(k).
- If your device cannot be found in the product classification database because it is a new type of device and should be classified as a Class III device because of the level of risk it presents*.
Class III devices support or sustain human life, are of substantial importance in preventing impairment of human health, or present a potential and unreasonable risk of illness or injury.
Note that if your device is a new concept without a substantial equivalent, but does not present the level of risk of a class III device, it may be eligible for the De Novo process as a class I or class II device.
PMA vs 510(k)
Not only are PMA and 510(k) processes applicable to different types of devices, they have different purposes.
510(k): A 510(k) is intended to demonstrate that the device for which approval is being sought is as safe and effective as a currently marketed device that does not require a PMA.
PMA: A PMA is intended to prove that a new device is safe and effective for the end user. A PMA is much more detailed and in-depth than a 510(k). Device manufacturers are typically required to present human clinical trial data, in addition to laboratory testing data.
The difference in complexity between a PMA and 510(k) also affects the time needed to process the submissions. The FDA typically accepts or rejects a 510(k) submission within 30-90 days, at which point the device is posted to the FDA’s 510(k) database. A PMA submission can take up to 180 days to be processed, at which point the FDA can approve or deny the application. The FDA may also issue an “approvable” or “not approvable” letter, which the applicant can choose to respond to, thereby adding time to the submission process.
PMA application methods
There are a number of types of PMA application methods. While most devices which require a PMA will follow the traditional process, be sure to verify that you are using the correct application process to maximize your chances for success and avoid unnecessary delays:
Traditional PMA
The most common method for attaining FDA clearance for Class III devices, the traditional PMA is the appropriate option for most devices that have completed clinical testing.
Modular PMA
The modular PMA is the appropriate application method for devices that have not yet completed clinical testing. Applicants complete individual “modules,” with final confirmation granted once all sections are completed. For additional information on specific requirements of a modular PMA, read the FDA’s Premarket Approval Application Modular Review.
Product Development Protocol
Use the Product Development Protocol (PDP) with medical devices that are based on well-established technology. The PDP process for gaining market approval merges the clinical evaluation and development of information, and involves an agreement between the manufacturer and the FDA. The process provides the advantage of early predictability for the manufacturer and allows early interaction that can identifyFDA concerns as soon as possible in the development process. Because the PDP identifies the agreed upon design and development details, a completed PDP is considered to have an approved PMA. For additional information, read more about the FDA’s PMA Application Methods.
Humanitarian Device Exemption
A Humanitarian Use Device (HUD) is specifically defined as a device intended to benefit patients that are affected by a disease or condition that affects less than 8,000 individuals in the U.S. per year. TheHumanitarian Device Exemption (HDE) approval process is designed to encourage clinical activity around rare conditions, and does have certain restrictions, including:
- After receiving HDE approval, a HUD is eligible to be sold for profit only if the device is intended to address a disease or condition that occurs primarily in pediatric patients, or occurs in pediatric patients in small numbers.
- If an HDE is approved to be sold for profit, the FDA will determine an annual distribution number(ADN). Any devices sold beyond the ADN limit are required to be sold for no profit.
For more information see the FDA’s explanation of the Humanitarian Device Exemption.
CBER Submissions
There are two centers within the FDA responsible for evaluating medical devices. While the majority of devices will go through the Center for Devices and Radiological Health (CDRH), some will be managed by The Center for Biologics Evaluation and Research (CBER). CBER regulates medical devices related to blood and cellular products, including blood collection and processing procedures as well as cellular therapies. This ebook focuses on submissions made through the CDRH, but you can view CBER Regulatory Submissions – Electronic and Paper for more information on the CBER process.
To continue reading this eBook, including a walk through of the different types of required and optional FDA meetings and communications, a detailed list of the contents of a traditional PMA submission, and an overview of quality management system requirements, please register to download the full version.
An overview of 21 CFR Part 11 regulations for medical device companies
What is 21 CFR Part 11?
21 CFR Part 11 refers to the federal regulation that address electronic records and electronic signatures associated with FDA requirements. This single, relatively small, part of the Code of Federal Regulations is extremely significant for companies with FDA-regulated products because it impacts every document signature, electronic file, and FDA submission. Codified in 1997, interpretations of this FDA-issued regulation continue to be debated and re-evaluated as the technology supporting electronic records and signatures changes. In this article, we’ll discuss the regulation and generally accepted interpretations.
Note that discussions and statements in this document are our observations only and should not be taken as fact. You can refer directly to the regulation here.
Part 11: General Provisions
The General Provisions section of 21CFR11 addresses the scope of the regulation, when and how it should be implemented, and defines some of the key terms used. It states that the purpose of Part 11 is to define the criteria under which electronic records, electronic signatures, and handwritten signatures attached to electronic records are equivalent to, and as reliable as, handwritten signatures on paper documents.
Fundamentally, any record that is maintained, used, or submitted under any FDA records regulation is subject to Part 11, and the FDA will accept electronic records in lieu of paper records if an organization can prove that their records and systems meet the Part 11 requirements.
The General Provisions subpart also sets forth a number of definitions, and we’ve listed the ones that are most significant to our discussion here:
- Closed System: A computer system or software whose access is controlled by the same people who are responsible for the information stored in the system. Because the opposite of a closed system, and “open system,” is subject to additional scrutiny be sure that you are able to thoroughly explain and provide documentation for a decision to classify your system as a “closed system.”
- Open System: A computer system or software whose access is not controlled by the same people who are responsible for the information stored in the system.
- Digital Signature: An electronic signature created in a manner that can be verified, ensures the identity of the signer, and maintains the integrity of the document and signature. This often involves the use of cryptography and/or biometric data.
- Electronic Signature: Symbols that represent a legally binding equivalent to an individual’s handwritten signature (as adopted and authorized by the signer).
Part 11: Electronic Records
The Electronic Records section sets forth the requirements for administration of closed and open electronic record-keeping systems, then discusses signature manifestations and requirements for establishing a link between signatures and records.
Part 11 defines a “closed system” as any computer system in which the users controlling access to the system are the same people who are responsible for the data in the system. Today, most systems can be classified as closed systems, but take special care to document control procedures around software that is hosted offsite or classified as a SaaS solution.
This section of the regulation deals with the controls that need to be in place for all applicable electronic record systems by defining:
- Procedures to ensure that all electronic records are authentic, have integrity, and can ensure confidentiality (where that is appropriate).
- Validation requirements for systems that maintain electronic records to ensure that all records are accurate, reliable, and that the system performs consistently according to regulatory requirements.
- Audit trail requirements for all regulated records to ensure a complete history of all changes to records are maintained.
- Controls around system access and document signatures.
Part 11: Electronic Signatures
The Electronic Signatures section defines the components of electronic signatures and the required controls and procedures necessary for using them.
In general, an organization must be able to demonstrate that electronic signatures:
- Are unique to each individual, and that the individual assigned an electronic signature has had their identity and level of authorization verified.
- Must be based either on biometric data (such as fingerprints) or made up of two distinct pieces (ie: a User ID and password)
- Require appropriate controls to ensure that they are verified periodically, cannot be used by someone other than the intended user, and are immediately deactivated if compromised in any way.
Practical application of 21CFR Part 11 for regulatory affairs professionals
21 CFR Part 11 is a critical regulation, and one that can be open to interpretation. Below, we cover some of the key areas that should be of concern for RA professionals. This is an overview of key areas only, and should not be taken as complete instruction or guidance for 21CFR part 11 compliance.
System compliance and validation
Any system that you are using to store electronic records that fall under FDA regulations needs to be compliant with Part 11. This includes everything from spreadsheets to full-featured RIM and document management systems.
Software vendors will often document how their systems are developed to be compliant, and may even support system validation during implementation - but it is ultimately the responsibility of the user organization to ensure that their systems and processes are compliant with Part 11. System validation is the process of documenting that your system meets all of the Part 11 requirements. Software vendors can support this process by ensuring that their systems are built on a highly secured infrastructure that can be demonstrated and proven.
The Rimsys system was built from the ground up to meet the stringent requirements of not only 21 CFR Part 11, but other industry standards and good practices guidelines (GxP). We have put in place a rigorous validation program, built by industry experts and supported by a secure and well-documented infrastructure. For more information, visit the Rimsys Security and Privacy page.
Audit trails
Audit trails are the required system logs that track the who, when, and what of every change made to data that falls under Part 11. Audit trails should be generated and time-stamped by the system, with no ability for users to change that information. Audit trails serve two purposes under 21 CFR Part 11:
- To demonstrate that documented policies and procedures are being followed, including that only users with the appropriate authority are managing data.
- To prove that data retention policies are being adhered to (see below).
At any time, you should be able to view the history of any record, from a Design History File to a submission document, in order to determine what changes have been made, when they were made, and by whom.
Record retention
21 CFR Part 11 specifies that electronic records must be protected and readily available throughout the defined record retention period. Additionally, 21 CFR Part 820 specifies that records related to the quality, manufacturer, regulatory submissions, or any other data that falls under FDA regulation, should be maintained for the life of the medical device and for a minimum of two years from the date of first commercial distribution. This is often referred to as “cradle to grave” tracking.
This means that regulatory professionals need to not only be aware of their company’s record retention policy, but need to ensure that any system being used to track regulatory submissions or other data subject to audit meets Part 11 and Part 820 requirements. Note that record retention requirements apply also to paper records where they are the source document.
Electronic and digital signatures
An important piece of 21 CFR Part 11 is its definition of electronic and digital signatures. “Electronic signature” is used to define any set of symbols that are used in place of a handwritten signature, whereas a “digital signature” is an electronic signature based on methods that ensure the identity of the signer where the integrity of the data can be verified. A digital signature can be based on biometric data (such as fingerprints) or secure user IDs and passwords that are controlled to ensure only one authorized user can use the signature.
As a regulatory affairs professional, you should ensure that:
- Everyone on your team who needs to sign documents has their own unique digital signature and understands the importance of protecting it. Sharing of electronic credentials is a common FDA audit observation. Also ensure that users who are not required to sign documents have appropriate access to data to discourage other users from sharing login credentials with them.
- You are following your company’s policies concerning electronic signature audits so that passwords remain updated and strong and signatures are revoked when a user leaves or changes positions.
- You immediately report any possible loss, theft, or sharing of user credentials or devices that generate identification codes.
While 21 CFR Part 11 is usually considered more of a “quality regulation,” it is important that regulatory teams within medical device organizations fully understand this regulation and its compliance implications. To learn more about the regulations, click below to read our regulatory brief.

RIM - Master data management for RA teams
Large medtech companies often have data stored in multiple ERP, PLM, and eQMS systems due to mergers, acquisitions, and siloed growth within product teams and departments. While segmented data can cause issues for everyone, it provides particularly concerning obstacles for regulatory affairs teams. RA teams in large organizations typically manage multiple product lines with various levels of classification across many global markets. When product and registration data is not centralized, regulatory teams will not only encounter significantly more complex processes related to managing and controlling data properly, but will also struggle to find and organize the data needed for submissions, license renewals, and other standard RA activities.
Regulatory data management issues without RIM
- Maintaining validation records for multiple systems: In the highly regulated world of medical technology, manufacturers are required to fully validate any system used to design, develop, or manufacture a medical device. Among other things, manufacturers must be able to demonstrate that only the current, approved version of a device can be manufactured. System updates and other changes trigger a re-validation process, which becomes increasingly complex as the number of systems increases. Not only does the system that is being changed need to be validated again, but any other system and process that is using data from the updated/changed system may need to be validated again as well. Issues with data integration between systems is a common finding during quality and regulatory audits.
- Ensuring data accuracy: As mentioned above, validating systems becomes exponentially more complex as the number of systems increases. In cases where the same data is stored in more than one system, the possibility exists that the data is not synchronized in real-time. Whether data is automatically transferred between systems or requires manual data entry or integration steps, each integration point is a possible point of failure. Regulatory and quality teams need to ensure that they identify the “source of truth” for each piece of data that is duplicated and that they can demonstrate the processes that ensure data integrity is being maintained.
- Managing user access: Managing user permissions in large systems, such as ERP solutions, often involves setting specific permission levels for a large number of detailed system functions. Users with access to information in one system may not have access to the same information in another system, causing auditing issues and creating difficulty in administering user credentials. For example, does a user have access to add regulatory documentation, such as EU MDR technical files or medical device certificates, into the system? If not, many companies end up circumventing their own systems by also using SharePoint or other shared drives to store updated files – where they may get lost or overlooked.
- Establishing system-related processes: Establishing and maintaining processes for system issues, downtime, updates, and other regular maintenance is impacted by the number of systems and the ways in which they are integrated. Regulatory teams won’t control these processes for non-regulatory systems, but may require access to data in these systems for time-critical tasks.
Regulatory workflow issues without RIM
Regulatory affairs professionals are familiar with the massive, color-coded spreadsheets that are often central to maintaining medical device registration information. While those spreadsheets work in some situations, without a centralized RIM system RA teams face two large challenges:
Software solutions not built for regulatory teams
- Spreadsheets are not the answer: While those large spreadsheets can be sufficient in smaller companies with a few products in a few markets, they quickly become unwieldy. Regulatory teams managing multiple submissions projects across global markets are compiling large amounts of information into specifically formatted portfolios for each country – a process that is difficult, at best, to manage with spreadsheets and pdf documents.
- Non-compliance risks: Regulatory teams that are managing data without a centralized RIM solution also run the risk of identifying changes and expiration dates too late, leading to higher consultant costs and the risk of non-compliant products.
- Missed opportunities: Most regulatory teams do an amazing job keeping multiple projects on track, products in compliance across the globe, and their company prepared for audits and inspections. What if, however, regulatory teams had access to a centralized regulatory system that could provide them with the information, and the time, to contribute to strategic product marketing and staffing decisions? We believe that an organization with a revenue-aligned, strategic regulatory team has a competitive advantage in the marketplace. Read more in our ebook, Regulatory Strategy as a Competitive Advantage.
Regulatory data in multiple systems
We know that 70% of regulatory teams spend at least half of their time on repetitive administrative tasks. Much of this is because the data they need is stored in multiple systems across the organization, with the same data often being stored in multiple places. This leads to an increased chance of outdated information being used, required data being missed, and difficulties in proving that the data management processes in place are sufficient for ensuring accuracy.
The information required by regulatory teams comes from teams throughout an organization, including product data from the engineering team, production and supplier information from the manufacturing team, quality records from the QA team, clinical trial data from the clinical team, and more. This is all in addition to the regulatory submissions, changes, and agency communications managed by the RA team themselves. Without a centralized system to record and reference all of this data, regulatory teams are left to a lot of research, searching, and duplication of efforts across the team.
Data warehouses as an option
In cases where there are multiple, enterprise-level systems sharing the same data, a data warehouse is often used. Data warehouses provide a centralized system in which to store data and maintain that single “source of truth” that all systems can pull data from. However, these systems can be extremely expensive and complex to set up and maintain. They normally require a team of consultants or internal staff to manage the setup and maintenance of the warehouse, including complex ETL (extract, transform, and load) workflows. These workflows are required because data stored in multiple systems will almost never be in the same format and will need to be “transformed” before being loaded into the data warehoused.
In addition, data warehouses are not typically updated in real-time and require that data cleaning and verification procedures run before data is uploaded. This makes a data warehouse a poor option for data that is needed for daily workflows and processes, such as UDI data management.
Regulatory Information Management (RIM) systems as a better option for master regulatory data management
Regulatory Information Management (RIM) systems, such as Rimsys, are designed to be the central source of truth for regulatory information. Purpose-built for regulatory teams, RIM solutions are powerful because they provide:
Centralized, product-centric, regulatory data
Information and data that is specific to regulatory activities can be stored and accessed directly in the RIM solution. This includes information such as submission documents, registration certificates, product references to standards and essential principles, and regulatory authority communications. The RIM solution is the original “source of truth” for this information.
As a result, RIM solutions provide regulatory teams with control over critical data, such as “available to sell” flags at a product version and country or market level. This ensures that the regulatory team is managing a product’s availability to be sold, market-by-market, based on its regulatory status in each market.
Integrated data
Regulatory teams require data from across the organization to manage submissions and other regulatory activities. A strong RIM solution will provide for integration with PLM, eQMS, eDMS, ERP, and other solutions that typically house information used by regulatory teams. For example, the design and engineering teams will likely utilize a PLM system to manage product details and revisions. While that data is needed by the regulatory team, it is owned by the design and engineering teams and belongs in their PLM system.
Rimsys provides secure API endpoints that simplify integration with nearly any system with a REST API.
Rimsys also simplifies compliance with 21CFR part 11 and other regulations by providing complete and easy-to-read activity logs for all actions taken within the software.
To learn more about how Rimsys can be your master data management system, schedule a time with one of our product experts to see Rimsys in action.

EU country-specific medical device registration requirements
There are 27 member states that belong to the European Union (EU), along with additional countries that participate in the European Economic Area (EEA) and the EU’s single market. One of the benefits of belonging to the EU is the unification of regulations for medical devices and in-vitro diagnostics. As you know, registering medtech devices (ultimately known as applying the CE Mark) is a complex process. Applying the CE Mark allows your devices to easily be imported and sold throughout Europe.
Some of the member states and those participating in the single market require additional registration steps beyond those required by the EU for class IIa, class IIb, and class III medical devices. In general, a medical device manufacturer is required to submit a registration form and/or enter information in the online database before placing the product on the market. Typically, this notification includes the upload of a localized label, instructions for use, Declaration of Conformity, and the CE certificate.
The additional registration requirements apply to manufacturers outside of the EU who wish to market devices in an EU member country. Most markets will also have additional or different registration requirements for local Authorized Representatives and Manufacturers. Once EUDAMED is fully implemented, the assumption is that most of these country-specific registration requirements will be removed.
The table below lists all 27 EU member states, along with additional countries that participate in the EU single market. This table is for reference only – Regulatory professionals are urged to consult country Competent Authority websites for country-specific requirements.
* Countries not in the EU
+ Devices supported by Finnish distributors to hospitals and retailers require notification.
++ Registration may be required if an importer, authorized representative, or manufacturer located in Germany is placing the product on the market for the first time.
Note: Specific requirements for local economic operators are not included here and may include both additional entity and device registration requirements.
FDA transition plans for Covid-19-related medical devices
New guidance
The FDA has issued two final guidance documents intended to assist with transition plans for medical devices that are currently being distributed under emergency use authorizations (EUAs) or that fall under specific policies issued to support the response to the COVID-19 pandemic. The agency states that they recognize that it will take time for manufacturers and others to adjust to “normal operations” as policies adopted during the pandemic come to an end. However, they are recommending that organizations move quickly to plan their regulatory strategy and engage with the agency where necessary.
The two guidance documents are:
- Transition Plan for Medical Devices Issued Emergency Use Authorizations (EUAs) Related to Coronavirus Disease 2019 (COVID-19) Guidance
- Transition Plan for Medical Devices that Fall Within Enforcement Policies Issued During the Coronavirus Disease 2019 (COVID-19) Public Health Emergency
Transition periods
Advance notices will be published in the Federal Register for each EUA declaration 180 days prior to the termination of the EUA.
For devices that fall within enforcement policies issued during the COVID-19 public health emergency (PHE), a 180-day transition period is also available and will begin following the expiration of the section 319 PHE declaration. Manufacturers should refer to the following “list 1” COVID-19 public health emergency enforcement policies for more detail:
- Digital pathology devices
- Imaging systems
- Non-invasive fetal and maternal monitoring devices
- Telethermographic systems
- Treating psychiatric disorders
- Extracorporeal membrane oxygenation and cardiopulmonary bypass devices
The FDA’s stated intent with this guidance is to, among other things, “help avoid disruption in device supply and help facilitate compliance with applicable FD&C act requirements after the termination of the relevant EUA declaration…”
Guiding principles
The following guiding principles are taken directly from the guidance documents listed at the beginning of this article, and they are the same in both documents.
- This guidance is intended to help facilitate continued patient, consumer, and healthcare provider access to devices needed in the prevention, treatment, and diagnosis of COVID19.
- FDA believes the policies and recommendations in this guidance will help to ensure an orderly and transparent transition for devices that fall within the scope of this guidance. FDA’s policies and recommendations in this guidance are consistent with the Agency’s statutory mission to both protect and promote the public health.
- FDA’s policies and recommendations follow, among other things, a risk-based approach with consideration of differences in the intended use and regulatory history of devices, including whether the device is life-supporting or life-sustaining, capital or reusable equipment, a single-use device, and whether another version of the device is FDA cleared or -approved.
- As always, FDA will make case-by-case decisions regarding the enforcement of legal requirements in response to particular circumstances and questions that arise regarding a specific device or device type. This may include FDA revising or revoking an EUA,29 requesting a firm initiate a recall (see 21 CFR 7.45), or taking other actions, including an enforcement action. Moreover, FDA may revise the enforcement policies and recommendations in the guidance, as appropriate.
Do not wait to submit marketing submissions
Manufacturers who intend to seek market authorization for devices currently under COVID-19-related EUAs should begin working on their market submission and transition implementation plan as soon as possible. The CDRH is encouraging organizations that want to continue marketing their device, and need a marketing submission, to take advantage of the full transition period, including submitting a pre-submission if needed. The pre-submission process allows for early interactions with the CDRH.

Nonconformance reporting for medical device manufacturers
Defining nonconformance
Very simply, a nonconformance occurs when a specification is not met. The FDA defines a specification in 21 CFR 820.3 as “any requirement with which a product, process, service, or other activity must conform,” and ISO 13485:2016 as a “need or expectation that is stated, generally implied, or obligatory.”
While managing nonconformance starts with fully defining specifications; it is the identification, tracking, and resolution of nonconformance that is a focus of medtech quality and regulatory teams and a requirement of both ISO 13485:2016 and the FDA’s 21 CFR Part 820 quality system regulation.
Identifying nonconformance occurrences
As part of a compliant quality system, medical device manufacturers should implement procedures to identify and address both major and minor non-conformances. Nonconformances may be identified through processes found in multiple subsystems that are part of an overall quality management system within the organization.
The systems and subsystems in which nonconformances are identified typically include:
- ERP
- Regulatory information management (RIM)
- Product lifecycle management (PLM)
- Document management
- Customer service / customer management
- Complaint handling
- Device history records
- Audit management
- CAPA
- Training/learning management
- Calibration/preventative maintenance
- Development change management
Evaluating nonconformance
Once a nonconformance is identified, it should be evaluated in a timely manner, and a determination made as to the disposition of any affected products. Requirements for additional investigation and reporting should also be identified. Based on the severity of the nonconformance and its effect on the safety and efficacy of devices being manufactured or already in the market, a CAPA (corrective/preventative action) record may need to be created. In the U.S., this is defined in the quality regulation 21 CFR Part 820.100.
To disposition a nonconformance, consider the following:
- Will the existing system detect the nonconformance if it recurs in time for remediation?
- How likely is it that this issue will recur?
- What is the impact of the non-conformance (i.e., could it affect patient health)?
Issues that are more severe or are more likely to recur should trigger a more immediate and comprehensive response.
Nonconformances that are escalated and handled under CAPA are based on risk and can include those that have or could have an impact on a product or process that is:
- Not easily corrected
- Recurring
- Severe
In addition, nonconformances that rise to the level of a CAPA require significant resources and typically result in a full project to identify root cause(s), containment, and corrective actions, and monitoring for effectiveness.
Nonconformances that don’t require a CAPA have simpler resolutions that include documenting actions taken to correct the issue (or justification for no action). If the issue is not recurring, there may be no other action required. For example, a nonconforming material received from a vendor may be a singular issue that was easily identified through existing inspection procedures and is not expected to recur. In this case, the material is returned to the vendor and no additional action is required.
Processes that are out of conformance are often resolved through improved documentation and/or additional user training. However, be sure that the true root cause of the nonconformance is identified as procedural nonconformances can signal additional issues.
Documenting nonconformances
An important part of nonconformance procedures is the nonconformance report (NCR) or other documentation procedures. Nonconformances are typically documented within the subsystem in which they were identified. Some organizations will have a nonconforming system in which issues originating from all subsystems are documented. Centralized nonconformance systems allow for trending and other analysis across all subsystems, the results of which may generate CAPAs.
The requirements for documenting a nonconformance may vary by subsystem. In general, however, nonconformance documentation records:
- The requirement/specification that was not met.
- The objective evidence supporting the determination.
- The action that is being taken to address the nonconformity.
Nonconformances are a common point of focus during quality audits by regulatory bodies, including the FDA, and should follow a well-documented process. Auditors will often try to determine if the quality system is functioning effectively by looking at self-identified nonconformances and comparing them to externally reported nonconformances. This is to ensure that nonconforming products were not released, or that the appropriate actions were taken to resolve issues in the field.
The importance of nonconformance reports
Nonconformances related to distributed products of higher risk result in nonconformance reports issued to government authorities through vigilance reporting, medical device reporting, and field action/recall reports. For example, the FDA requires that a medical device report be submitted within 30 days of a serious adverse event (see 21 CFR Part 803 Subpart E). Strong reporting procedures for nonconformances of all types are important in identifying trends, addressing issues before they become critical, and as part of a complete quality management system.
A nonconformance reporting procedure is only part of a strong quality system. Read An overview of 21 CFR part 820 and ISO 13485 overview for more information on establishing quality systems for medtech companies.

Regulatory strategy as a competitive advantage
This article is an excerpt from the Regulatory strategy as a competitive advantage ebook.
Table of Contents
- The regulatory revenue opportunity
- Regulatory responsibilities
- Limitations of the "cost-center" approach to regulatory affairs
- Regulatory as a revenue function
- Competitive advantage #1: Faster time to market
- Competitive advantage #2: Cost avoidance
- Competitive advantage #3: Out-pacing competitors
- Why invest in regulatory/revenue alignment?
- Getting started - 3 steps to move towards a revenue-aligned RA team
It is well known that medical technology (medtech) companies are highly regulated, given the potential risks their products present. Understanding and complying with the complex regulations in each country is, therefore, a necessary part of marketing and selling medical devices. To realize any revenue from a medical device, it must not only demonstrate compliance with all applicable regulations, it must also receive and maintain market clearance from each country in which it is to be sold. No market clearance means no revenue. Given the key role regulatory compliance plays in revenue attainment, regulatory teams, tools, and processes present a significant opportunity for differentiation for organizations willing to invest in them.
For the majority of medtech companies, however, regulatory departments have traditionally been treated as operational cost centers, with departmental improvements focused on cost reduction and efficiency improvements. Limited investment in people and tools, and limited interest in digital transformation, have left regulatory teams across the medtech industry underfunded and under-resourced.
This has led to great resourcefulness within the RA community, where most members can point to heroes within their team who worked long hours to meet a submission deadline, headed off a disaster by uncovering a pending expiration, created ad-hoc systems to organize information and streamline communication between the RA and QA teams for smoother audits, or have otherwise gone above and beyond their typical responsibilities.
Regulatory teams, however, have the potential to be a revenue-driving competitive weapon for companies that are willing to look at them a little differently and invest in regulatory performance above regulatory cost-effectiveness. Well-supported regulatory teams can provide a true competitive advantage by providing the resources and direction to:
- Capture market share by being first to market with novel devices.
- Avoid lost revenue by effectively tracking and planning for registration renewals/updates.
- Out-pace competitors and grow market share by adapting to regulatory changes more quickly and taking advantage of competitors’ non-compliance or inability to enter a new market.
We believe we are entering a new era for regulatory affairs within the medtech industry. One in which RA teams have a seat at the table when go-to-market, competitive positioning, and strategic decisions are being made.
In the medtech industry, regulatory affairs (RA) teams have a broad range of responsibilities across the product lifecycle:
Premarket regulatory strategy
Obtaining market clearance for a new medical device is the primary activity typically attributed to RA teams. It is not unusual for a regulatory team to be given market entrance projects with little warning, but ideally, the RA team would be brought in as early as possible to contribute to go-to-market discussions.
Premarket regulatory strategy, at a minimum, involves:
- Determining the most appropriate pathway to market approval. For example, a 510(k) or PMA submission in the U.S.
- Working with quality, product, and other teams to gather information needed for market submission.
- Establishing communication with applicable regulatory bodies and third-party approved auditors.
- Compiling and submitting required documentation for market approval. This includes managing follow-up activities, questions, and requests for additional information throughout the approval process.
Forward-thinking organizations often look to bring in RA teams even earlier in the process. As regulatory experts, RA professionals can provide unique insight into product development plans. In consultation with R&D teams, can help to refine product strategies, and steer development in areas that will reduce regulatory hurdles when new products are ready to be commercialized.
Maintaining regulatory compliance for existing products
While the primary focus of regulatory teams is often considered to be new market submissions, the majority of their time is actually spent on maintaining compliance for products that are already in-market. Even in situations where market registrations do not expire, constant vigilance is required to ensure that devices remain compliant with current regulations. These efforts take a considerable time for a typical RA team because information is often spread across disparate systems, where it can be difficult to find and confirm.
Maintaining regulatory compliance for approved devices includes:
- Staying on top of changing standards and making changes as required to existing technical files and other documentation.
- Submitting appropriate documentation updates when there is a change made that could potentially affect the efficacy or safety of the product, such as a material switch or facility change.
- Understanding pending regulatory changes and proactively addressing any that have an impact on devices currently in-market.
- Tracking registration expirations and preparing for timely re-submissions to ensure there is no lapse in market clearance.
Post-market activity
Post-market surveillance and vigilance activities are required by most countries and should involve the cooperation of the quality and regulatory teams. Ensuring that changing post-market reporting requirements are understood and complied with is an important regulatory responsibility.
Regulatory teams typically play a role in:
- Post-market surveillance of adverse events, complaints, and any issues associated with a device in the field.
- Assembling and submitting any required periodic safety reports to country/regional health authorities.
- Post-market vigilance and reporting of serious events to the appropriate regulatory agencies.
- Any required communication with regulatory authorities regarding adverse events or concerning trends in product quality.
Ask any RA professional, and they are likely to tell you that they work long hours and are often scrambling to meet looming deadlines...
To continue reading this ebook, download the full version.
Essential principles
What are Essential Principles?
Essential Principles (EPs) are requirements established by a country’s health agency. Medical device manufacturers need to prove that they comply with these requirements in order to sell their device in each country where they are required. This is often tracked in a burdensome table in which each requirement is explained by applicable standards and other items used to demonstrate compliance with each requirement. The manufacturer will link their evidence files to prove that they meet the requirement or provide an explanation as to why it is not applicable in their situation.
Think of this like cliff-notes for the submission and related documents. Submission documents, their locations, and explanations can all vary depending on the device type, manufacturer, and their processes.
What countries require Essential Principles?
Not every country requires EPs for their submissions. Some of the main countries that do require them include:
- The European Union – where they are called General Safety and Performance Requirements (GSPR)
- Australia
- Malaysia
- Singapore (accepts EU documentation in most cases)
- China
What do Essential Principles look like?
GSPR (General Safety and Performance Requirements) in the European Union are an example of Essential Principles requirements. The language in the GSPR comes directly from Annex 1 of the EU MDR of 745/2017 for medical devices and EU IVDR 2017/746 for in-vitro diagnostic devices. Medical device manufacturers are taking the text of this regulation, numbering and all, and documenting whether they apply to it, the standards that they apply to, and then providing their evidence.
Let’s look at an example that directly comes from EU MDR 2017/745, Regulatory text, Annex I, 7th requirement:
“Devices shall be designed, manufactured and packaged in such a way that their characteristics and performance during their intended use are not adversely affected during transport and storage, for example, through fluctuations of temperature and humidity, taking account of the instructions and information provided by the manufacturer.”
The validation of the Essential Principles for this particular requirement would be displayed in a table like the one below. Note that the description column in the table and in the EU MDR regulatory requirement are identical to each other.
These tables change constantly, and it is a large administrative burden on the regulatory professional to quickly identify changes, perform a gap analysis (check for changes and do testing if needed), and update the tables when required. In addition, we have seen the following issues caused by changing standards:
- Large companies can have hundreds to thousands of Essential Principles tables. Without a bulk upload, this can take an incredibly long time to process all of those documents.
- Errors can occur with standards updates by missing a product that is associated to a standard.
- If a gap analysis is done too late and testing a product to a revised or new standard is required - your product might need to be blocked from a market for months, which could mean massive revenue loss.
- Accidentally missing a reference to new testing data because only the standard was updated.
Rimsys allows regulatory professionals to be notified of standard changes and even do bulk additions and deletions of documents, standards and certificates to your Essential Principles Tables, which can save regulatory professionals countless hours in administrative work. For more information on how one of our customers benefited from our Essential Principles tool, reducing their EP and GSPR maintenance by 99%, read our Bisco case study.
